National Renal Pathology E.Q.A. Scheme
Circulation Y
This document gives information on individual cases in
circulation Y of this scheme. It contains no personal details
of participants.
Cases included:
Y 272
Y 273
Y 274
Y 275
Y 276
Y 277
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: Y
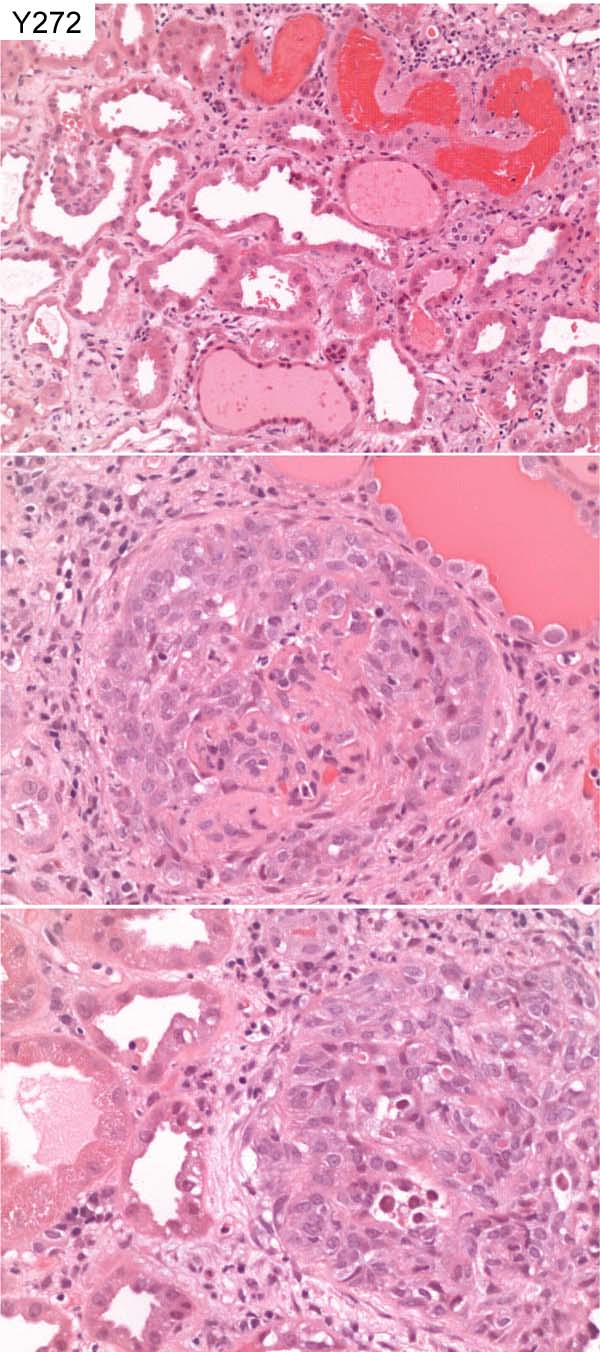
Case number: 272
....
Number of responses:83 . Date of analysis: 7 JUL 07
Clinical:
Male, 64 y.o. Known hypertension & ischaemic heart disease. Acute on
chronic renal failure, creatinine inc from 140 - 1066. Haematuria,
arthralgia. ANCA +, PR3. ?vasculitis. On ACE inhibitors & NSAIDS. IF
showed small amount of IgA within paramesangium. Small amount of granular
IgG in a peripheral location. C3 shows non-specific staining. No other
immune reactants.
Specimen:
H&E
Diagnostic categories: Score:
1 Pauci-immune crescentic Gn / vasculitis 8.59
2 Henoch Schonlein nephritis / IgA nephropathy 0.54
3 Granulomatous interstitial nephritis 0.12
4 Crescentic Gn / IgA nephropathy 0.27
5 Wegener's glomerulonephritis 0.12
6 Crescentic glomerulonephritis NOS 0.24
7 Extracapillary proliferative glomerulonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.59
Secondary diagnoses and comments (if any):
Exclude ascending infection*1. EM*16. Silver stain*4. PAS*2. Need to see
IgA to judge significance *15. ATN too*7. Anti-GBM antibody?*1.
Insufficient material / not suitable for EQA*12.
Original report and further information (if any):
Necrotising glomerulonephritis consistent with ANCA-positive vasculitis.
Also acute tubular damage and haemorrhage. Choroic damage probably due to
longstanding hypertensive vascular damage.
Circulation: Y
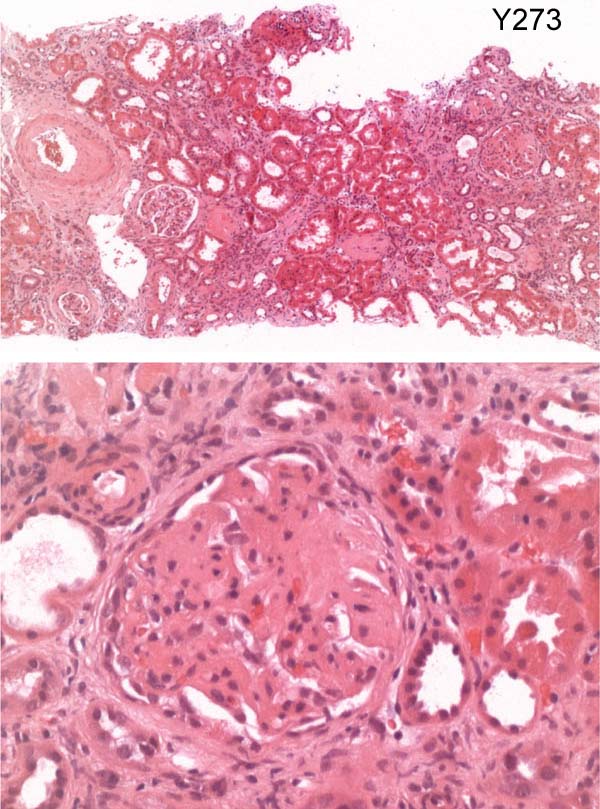
Case number: 273
....
Number of responses:83 . Date of analysis: 7 JUL 07
Clinical:
Female, 44 years old. Arthralgia and rash. Creatinine 150, MPO >100, ANA+,
pANCA+. Immunofluorescence: IgA/M/G, C1q, C3 all positive. EM not
performed.
Specimen:
H&E
Diagnostic categories: Score:
1 SLE class III 5.30
2 SLE Class II 2.05
3 SLE class IV 1.33
4 SLE NOS 0.60
5 Mesangial proliferative Gn (SLE not mentioned) 0.12
6 Henoch Schonlein purpura 0.12
7 Gn ?SLE 0.12
10 Specific diagnosis not possible, ?SLE 0.36
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.30
Secondary diagnoses and comments (if any):
Further lupus serology (e.g. anti-dsDNA)*11. Silver stain (for
subclassification*6)*14. PAS*4. EM*14. More details/pictures of IF*12.
More clinical info*5. Drug history?*2. Oxalate crystals noted*1.
Unsuitable for EQA*5.
Original report and further information (if any):
Circulation: Y
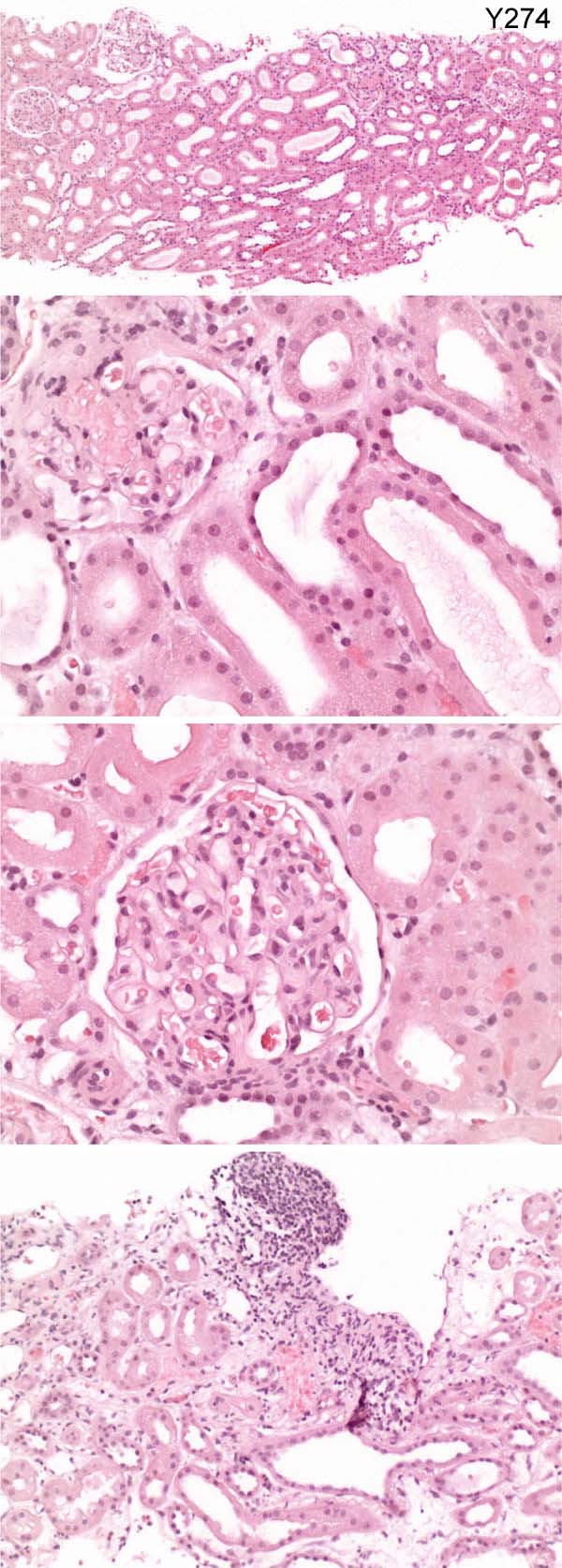
Case number: 274
....
Number of responses:83 . Date of analysis: 7 JUL 07
Clinical:
Male, 27 years old. "Coryzal" symptoms for one month. Creatinine on
presentation 608. No other significant haematological or immunological
findings. IP: Negative. EM: No glomeruli.
Specimen:
H&E,
Diagnostic categories: Score:
1 Acute tubular necrosis 5.59
2 Normal (by light microscopy) 1.20
3 Sickle cell disease 0.22
4 HUS 0.02
5 Tubulo-interstitial nephritis 0.43
6 Not diagnostic 1.45
7 FSGS 0.26
8 Minimal change nephropathy 0.22
9 Hereditary nephropathy 0.09
10 Others- post-infectious, HIVAN... 0.52
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.59
Secondary diagnoses and comments (if any):
Unsuitable for EQA*39. EM on material from paraffin block*5. Silver*5.
PAS*2. More clinical info.*7. Proteinuria?*2. Exclude myoglobinuria*1.
TIN too*1. Tubular damage insufficient to explain ARF*6. Drug related?*4.
Original report and further information (if any):
Acute tubular insult. No true necrosis. No significant glomerular changes.
Creatinine peaked at 608, then completely normal 2-3 months later, with
supportive therapy only.
Circulation: Y
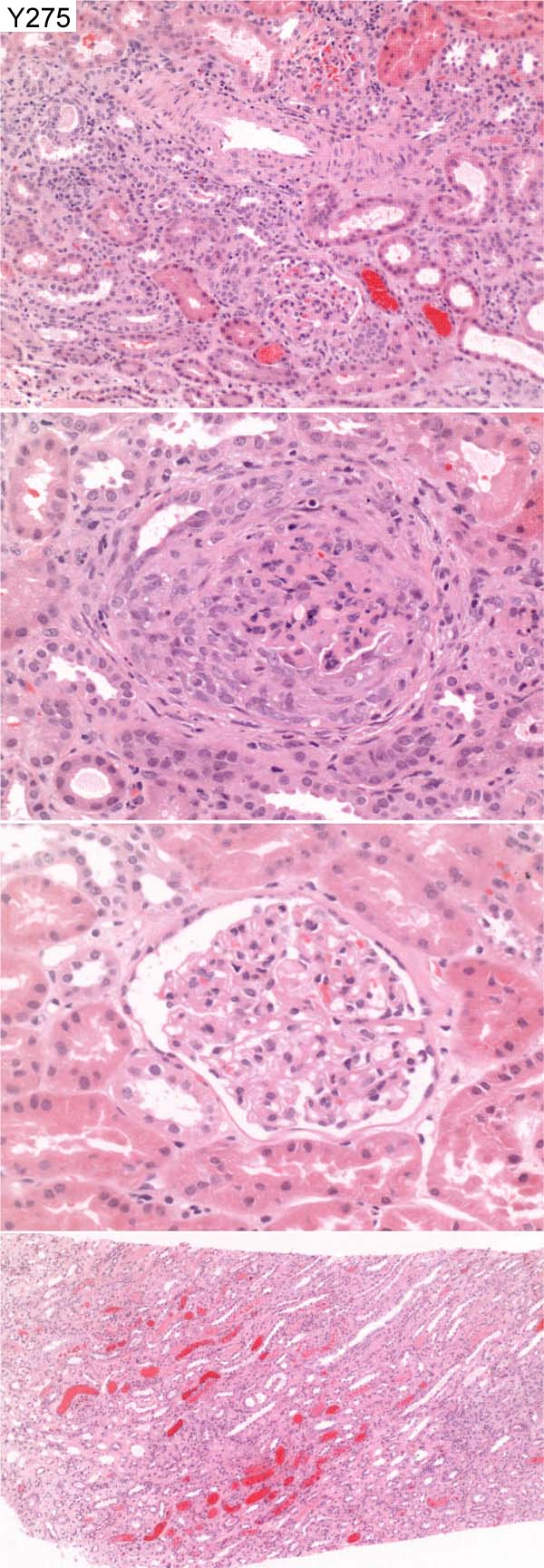
Case number: 275
....
Number of responses:83 . Date of analysis: 7 JUL 07
Clinical:
Female, 17 years of age. Six weeks haemoptysis. Anti GBM positive in the
blood test. Raised creatinine - 114. Immunofluorescence - IgG 3+ linear GBM
staining with some C3.
Specimen:
H&E
Diagnostic categories: Score:
1 Anti-GBM antibody disease / Goodpasture 9.76
2 Probable vasculitis, not diagnostic 0.12
3 Diffuse endocapuillary glomerulonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.76
Secondary diagnoses and comments (if any):
ANCA*2. Silver*4. MSB*2. PAS*1. ANCA?*4. Prominent interstitial
eosinophils ?TIN*2. Light micro. not typical of anti-GBM disease*3. Early
/ mild disease*6.
Original report and further information (if any):
Anti-GBM glomerulonephritis with clinical features of Goodpastures
syndrome. Treatment (immunosuppression and plasma exchange) was
successful.
Circulation: Y
Case number: 276
....
Number of responses:81 . Date of analysis: 7 JUL 07
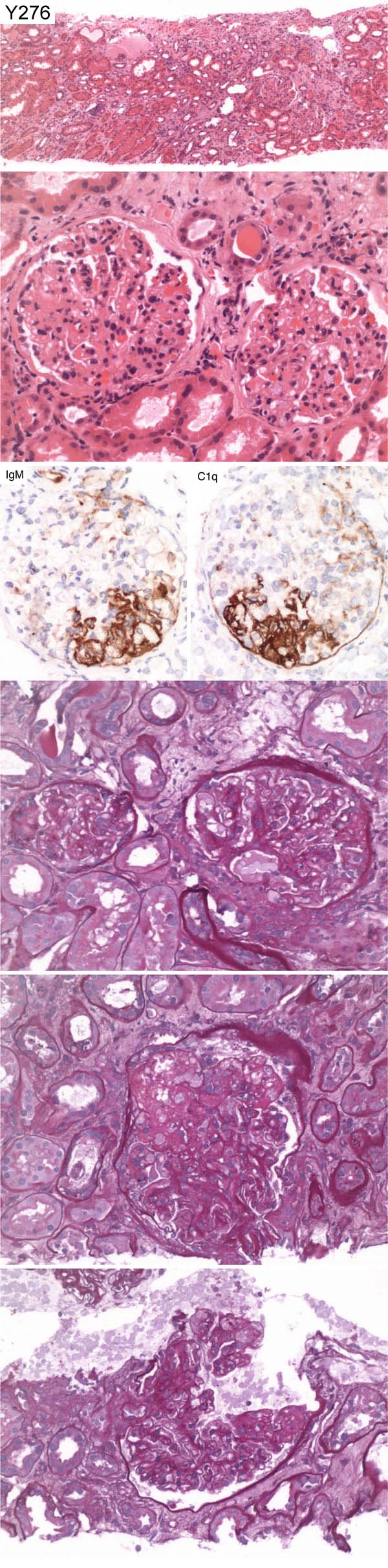
Clinical:
Male, 62 years old. Alcoholic liver disease and nephrotic syndrome with a
urinary protein of 5g/24hrs. EM shows patchy effacement of podocyte foot
processes and focal areas show wrinkling of basement membranes. No electron
dense deposits seen.
Specimen:
H&E, PAS, Photo's of C1q and IgM
Diagnostic categories: Score:
1 Primary FSGS 7.70
2 FSGS (collapsing / cellular form) 0.56
3 C1q nephropathy 0.07
4 FSGS (Tip variant) 0.48
5 Diffuse mesangial proliferative Gn 0.37
6 Diabetic glomerulopathy 0.12
7 Minimal change nephropathy 0.17
8 Focal Segmental Glomerulonephritis 0.25
9 Mesangiocapillary Gn 2ry to cryo. 0.12
10 Focal proliferative glomerulonephritis 0.15
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.70
Secondary diagnoses and comments (if any):
Secondary to liver disease?*3. Was IgA negative?*3. Not diagnostic /
unsuitable for EQA*4. Clinical info.*1. Silver stain*3. PAS*1. . Exclude
SLE*1. Exclude diabetes*2. Slides missing*3.
Original report and further information (if any):
Focal segmental glomerular sclerosis.
Circulation: Y
Case number: 277
....
Number of responses:74 . Date of analysis: 7 JUL 07
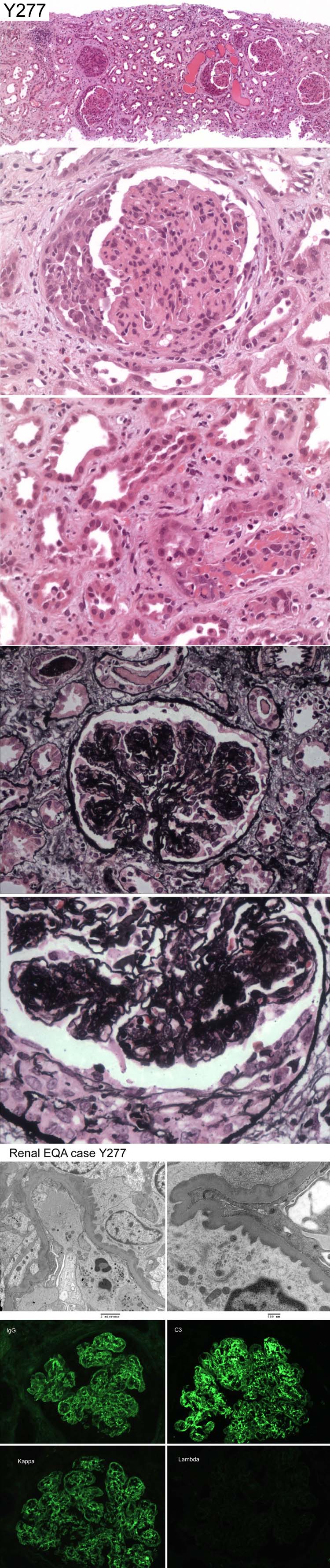
Clinical:
FOR EDUCATION AND INTEREST ONLY. Male, 65 years old. Acute Renal Failure.
Creatinine 124 in May, now 837. All immunology negative. Urine blood +++
protein +++ Initial presentation before ARF was nephrotic. IF for IgA and
IgM negative.
Specimen:
H&E, Silver: EM, IF of IgG, C3, Kappa & Lambda
Diagnostic categories: Score:
1 Monoclonal immunoglobulin deposition disease 1.62
2 Mesangiocap./ prolif. Gn with monoclonal deposits 2.91
3 Light chain deposition disease 3.04
4 Myeloma kidney and proliferative Gn 0.14
5 Membranous Gn and monoclonal protein deposition 0.41
6 Crescentic change in membranous Gn 0.41
7 Non-amyloid immunoglobulin deposition disease 0.27
8 Post-infectious Gn 0.41
9 Mesangiocapillary Gn 0.68
10 Immunotactoid / Fibrillary Gn 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 3.04
Secondary diagnoses and comments (if any):
Also ? post-infective?*1. ATN too*4. Cryoglobulinaemia?*3. Amyloidosis?*
2. Urine/serum IEP*2. Skeletal survey*1. See KI 2004;65:85-96*1. Any
deposit on TBMs?*1. ANCA?*1. Anti-GBM?*1. Higher mag. /more EM*3.
Original report and further information (if any):
Monoclonal immunoglobulin deposition disease, light and heavy chains,
causing a mesangiocapillary pattern of glomerulonephritis. Subsequent
investigation confirmed monoclonal IgG kappa paraprotein.
Links to cases in this document:
Top
Y 272
Y 273
Y 274
Y 275
Y 276
Y 277
Last updated: 7 JUL 07
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk