National Renal Pathology E.Q.A. Scheme
Circulation X
This document gives information on individual cases in
circulation X of this scheme. It contains no personal details
of participants.
Cases included:
X 266
X 267
X 268
X 269
X 270
X 271
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: X
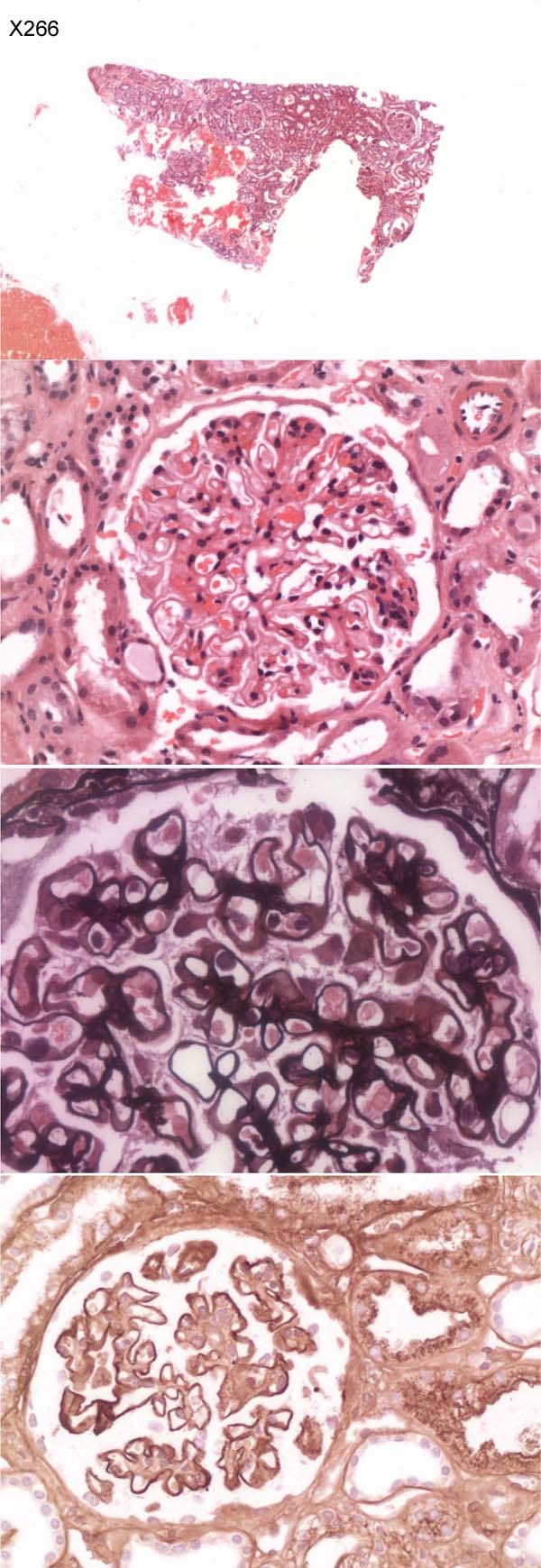
Case number: 266
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
79 year old female. Nephrotic syndrome. 5.8g proteinuria. Normal renal
function. Negative immunology. EM showed foot process effacement with
numerous small/medium subepithelial electron dense deposits with variable,
often small, spikes. Increase in mesangial matrix. No mesangial deposits
identified.
Specimen:
H&E, Jones silver and photo of IgG
Diagnostic categories: Score:
1 Membranous glomerulonephritis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Exclude renal vein thrombosis*2. Rest of immunoperoxidase?*2. Exclude 2ry
membranous*6. EM photos*1. Congo red*1. EM*1. Photo not present (but
didn't bother to tell Organiser!)*3
Original report and further information (if any):
Early membranous glomerulonephritis. The possibility of lupus should be
considered.
Circulation: X
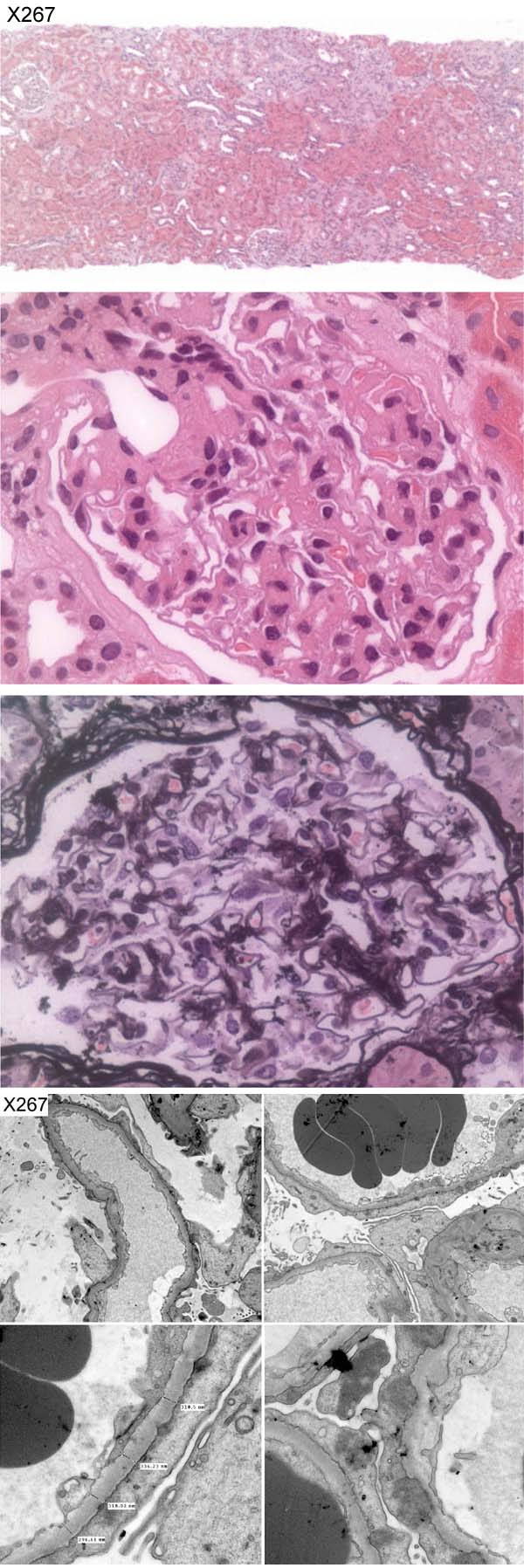
Case number: 267
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
67 year old female. Nephrotic, 10g. Normal creatinine. Albumin 16. ?
Membranous.
IF and IPx both negative.
Specimen:
H&E, Silver, photos of EM
Diagnostic categories: Score:
1 Minimal change nephropathy 5.95
2 Diabetic nephropathy 0.47
3 Membranous Gn 0.89
4 FSGS 2.04
5 Amyloidosis 0.22
6 FSGS with possible early membranous 0.12
7 Light chain nephropathy 0.06
8 Thin basement membrane disease 0.12
10 Unsuitable, no diagnosis offered 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.95
Secondary diagnoses and comments (if any):
More levels to exclude FSGS*many. Tubular atrophy noted*1. Congo red*8.
Clinical evidence of diabetes?*9. Repeat immuno as EM shows ?deposits*1.
Kappa & lambda IF *1. GBM ? thickened on EM*2. GBM thin on EM*1. ?'humps'
on EM*1. Higher magnification EM*2. Unsuitable for EQA*2.
Original report and further information (if any):
Minimal change nephropathy
Circulation: X
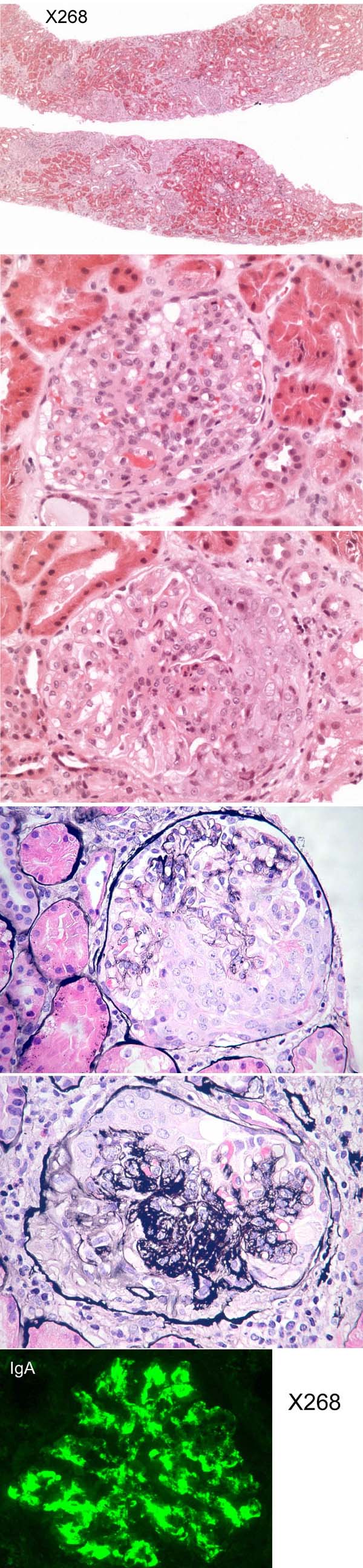
Case number: 268
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
26 year old female. Haemtoproteinuria. ?Cause.
Specimen:
H&E; Photos of IF for IgA, Silver x 2.
Diagnostic categories: Score:
1 IgA nephropathy 9.24
2 Henoch Schonlein disease 0.49
3 IgA neph. AND ANCA-associated disease 0.02
4 Prolif Gn; ?IgA, ?SLE, ?post-infective 0.24
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.24
Secondary diagnoses and comments (if any):
Rest of IF results?*11. EM*6. MSB*1. Exlcude lupus*3. Check ANCA*2.
ASOT*1. Clinical info. to distinguish IgA / HSP*6.
Original report and further information (if any):
Circulation: X
Case number: 269
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
15 year old male. Presented with microscopic haematuria and proteinuria for
8 months. Raised ASOT and IgA and decreased IgG. Immunohistochemistry for
IgA, IgG and C1q were negative.
Specimen:
H&E, PAMS & photos of EM, specials & IPx (2 sheets)
Diagnostic categories: Score:
1 Linear dense deposit disease (MCGn type II) 9.63
2 Dense membrane disease 0.12
3 Atypical post-infectious Gn 0.18
4 Focal segmental Gn 0.06
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.63
Secondary diagnoses and comments (if any):
Serum complement levels?*3. Factor H phenotyping & genotyping*1. Exclude
cryo*4. Resolving post-infective Gn too??*2. ?viruses in endothelial
cell?*1.
Original report and further information (if any):
Circulation: X
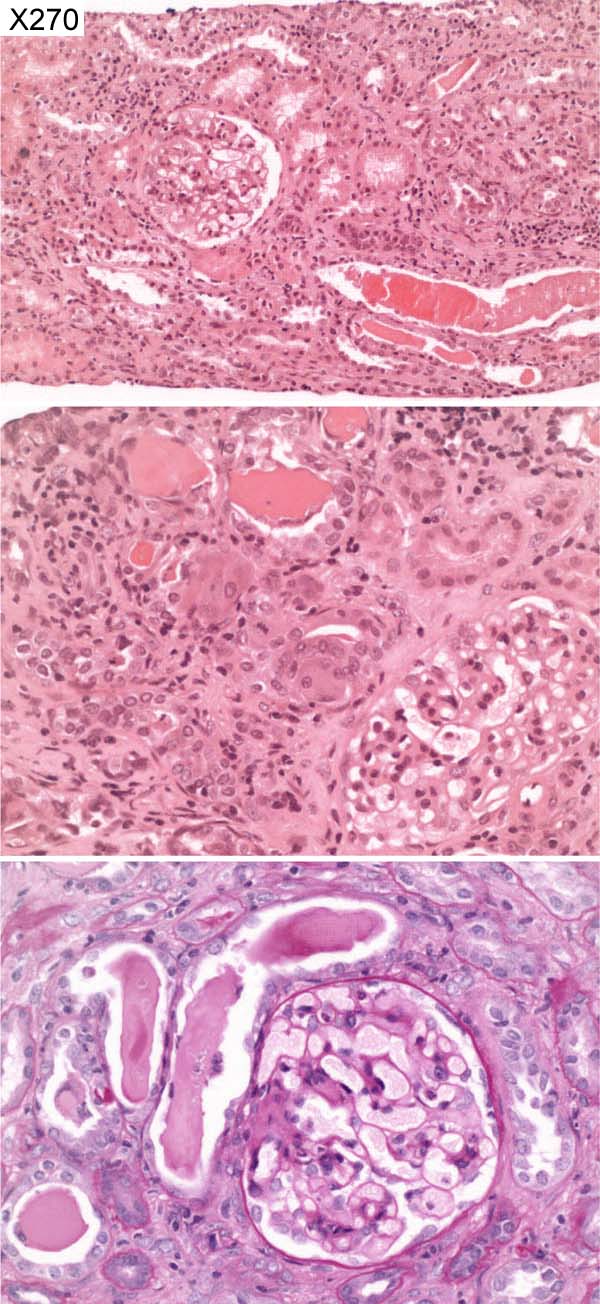
Case number: 270
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
Female, 58 years old. Myeloma August 2005, rapidly progressive renal
failure January 2006. ANA, ANCA anti-GBM, all negative. Not dialysis
dependant. IMF: IgM, IgG, IgA, C1q negative. C3: focal positivity in blood
vessels.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Myeloma cast nephropathy 9.88
2 Tubulo-interstitial nephritis (myeloma not mentioned) 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.88
Secondary diagnoses and comments (if any):
Clonality of infiltrate?*1. IF for light chains?*7. Clinical / radiological
/ serological tests for myeloma*6. Also light chain glomerulopathy??*1.
Congo red*10. EM*1. Exclude renal vein thrombosis*1. Drug history?*1.
Original report and further information (if any):
Circulation: X
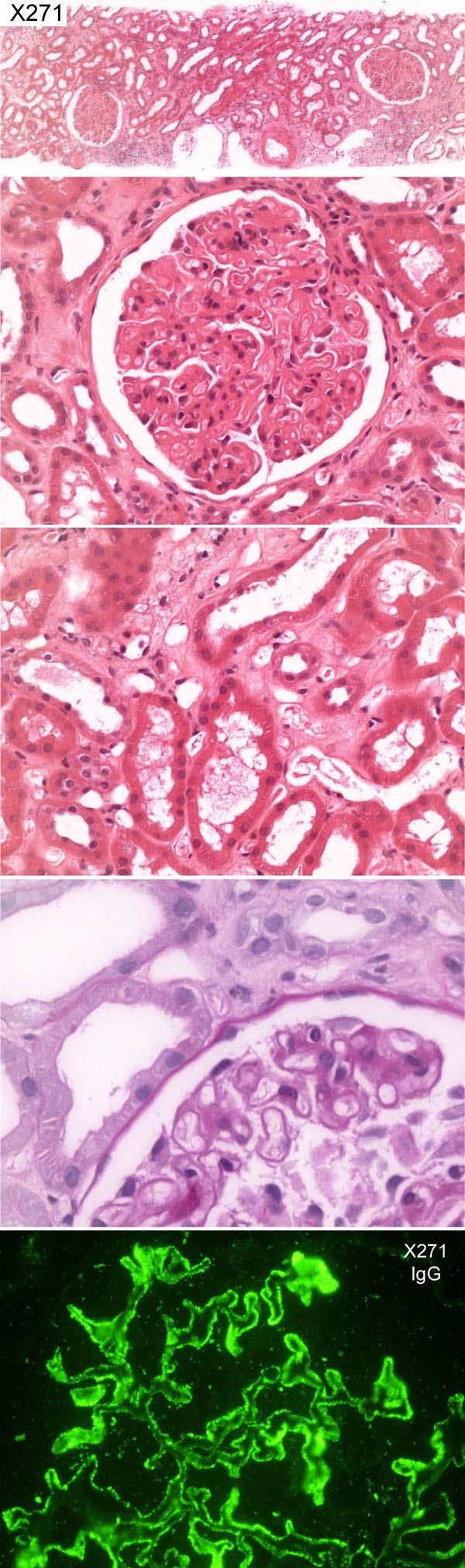
Case number: 271
....
Number of responses:82 . Date of analysis: 7 JUL 07
Clinical:
70 year old male. Nephrotic syndrome. High cholesterol. Previous
hyperthyroidism (treated with radio-iodine). COPD. Benign prostatic
hypertrophy. IF: 12 glomeruli showed bright diffuse global granular
capillary wall immunopositivity for IgG, light chains, C3d. Similar pattern
but weaker immunopositivity also present for C3, C1q. Negative for IgA,
IgM.
Specimen:
H&E, PAS and Photo of IgG
Diagnostic categories: Score:
1 Membranous glomerulonephritis 9.40
2 Light chain deposition disease 0.17
3 Fibrillary glomerulonephritis 0.18
4 Mesangiocapillary glomerulonephritis 0.06
5 Immunotactoid Gn 0.18
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.40
Secondary diagnoses and comments (if any):
Immuno for thyroglobulin in glomeruli*1. EM*15. Silver*11. CR*1. Exclude
renal vein thrombosis*1. Exclude myeloma*4. Exclude diabetes*1. Exclude
lupus*2. ATN too*1. Exclude 2ry membranous*3. Exclude radioiodine
treatment*1. Assume BOTH light chains positive?*5. (confusion about light
chain IF info. *several)
Original report and further information (if any):
Original diagnosis was membranous nephropathy.
Confirmed with electron microscopy showing typical subepithelial deposits.
Negative ANA, hep B, hep C screen. Continues with nephrotic range
proteinuria.
Links to cases in this document:
Top
X 266
X 267
X 268
X 269
X 270
X 271
Last updated: 7 JUL 07
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk