National Renal Pathology E.Q.A. Scheme
Circulation W
This document gives information on individual cases in
circulation W of this scheme. It contains no personal details
of participants.
Cases included:
W 260
W 261
W 262
W 263
W 264
W 265
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: W
Case number: 260
....
Number of responses:82 . Date of analysis: 19 JUL 06
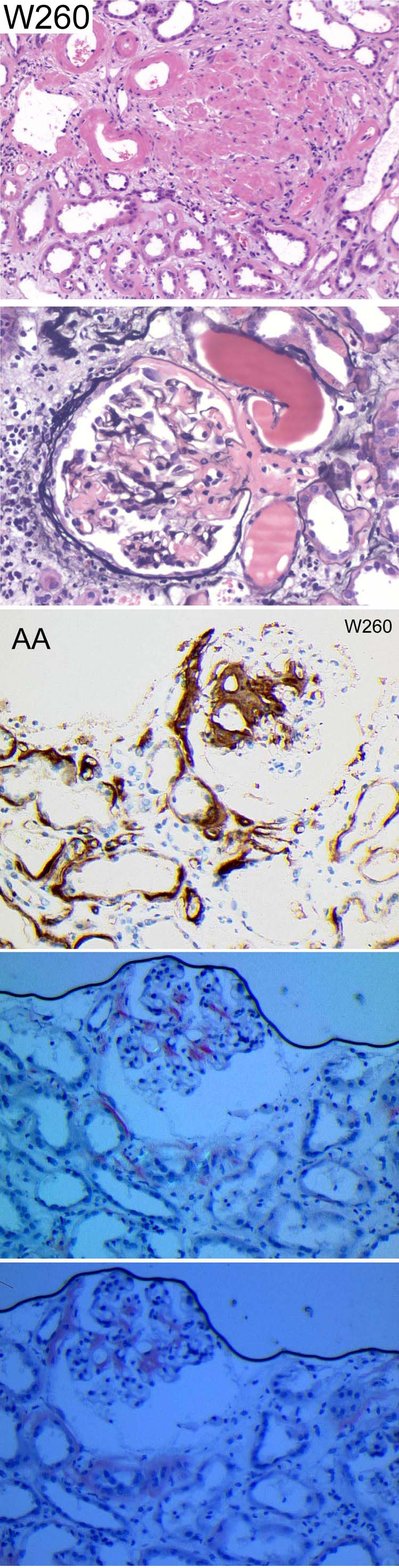
Clinical:
73 year old man with anaemia, renal failure and mild rouleux on blood film.
Specimen:
H&E, Silver, Photos of Congo Red and IPx for AA amyloid
Diagnostic categories: Score:
1 Amyloidosis 9.37
2 Cast nephropathy 0.02
3 Amyloidosis and cast nephropathy 0.61
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.37
Secondary diagnoses and comments (if any):
The photographs are atrocious*7. Actual slide of Congo red?*1. AA amyloid
*29. Tests for amyloid type*5. Myeloma casts too?*5. EM*5. PAS*2.
Underlying cause?*6. ATN too*18. Immunoelectrophoresis etc.*1. Serum EPG.
Creatinine?*1. Proteinuria?*2. Renal vein thrombosis?*1. Unsuitable for
EQA*5.
Original report and further information (if any):
AA amyloidosis (confirmed by National Amyloidosis Centre). No known
chronic inflammatory process or other predisposing condition.
Circulation: W
Case number: 261
....
Number of responses:82 . Date of analysis: 19 JUL 06
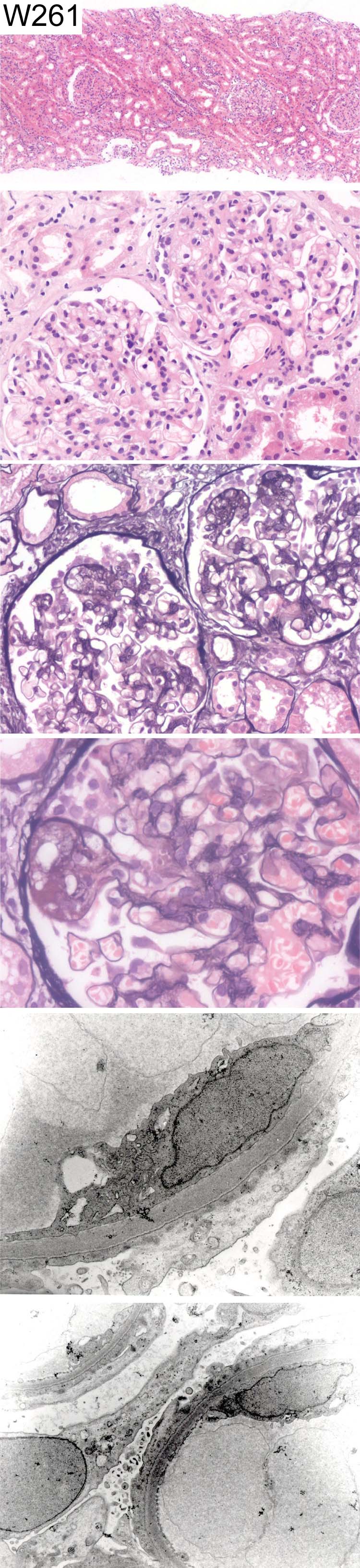
Clinical:
48 year old female. Presented with nephrotic syndrome. Normal blood
pressure and normal creatinine. IF showed trace positivity for IgM. IgG,
IgA, C3, C1q, Kappa and Lambda negative.
Specimen:
H&E, Jones Silver Photos of EM x 2
Diagnostic categories: Score:
1 Primary FSGS 5.62
2 Minimal change nephropathy 3.77
3 Minimal change with 'tip' lesions 0.37
4 Focal segmental proliferative glomerulonephritis NOS 0.12
5 IgM nephropathy 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.62
Secondary diagnoses and comments (if any):
Levels to look for segmental sclerosis*11. Larger/more EM images*5.
Consider diabetes*1.
Original report and further information (if any):
Focal segmental glomerulosclerosis; segmental sclerosis NOS and 'tip'
lesions.
Circulation: W
Case number: 262
....
Number of responses:82 . Date of analysis: 19 JUL 06
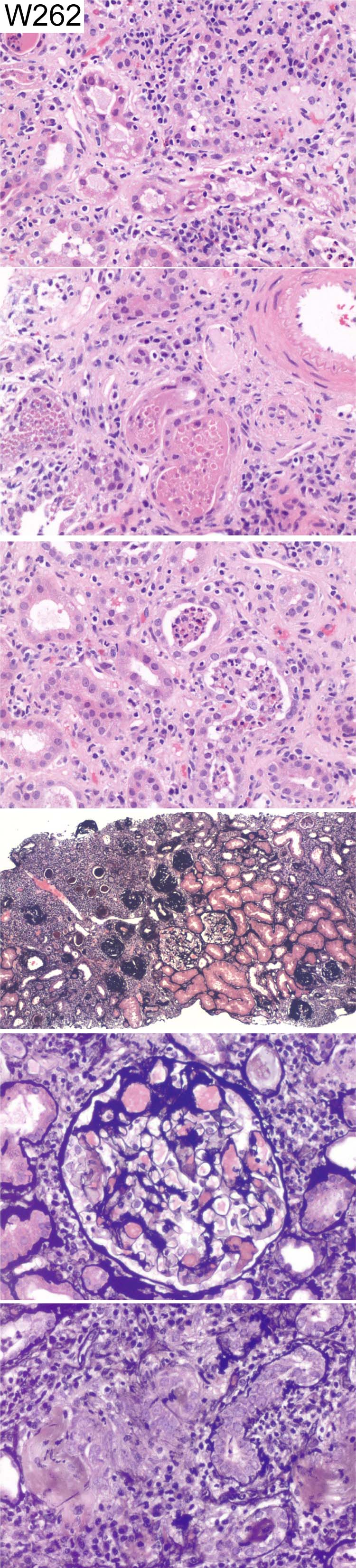
Clinical:
52 y.o female. Acute renal failure. Raised ESR. IF negative. EM no
significant abnormalities
Specimen:
H&E, PA silver
Diagnostic categories: Score:
1 Tubulo-interstitial nephritis (exclude infection) 5.00
2 Tubulo-interstitial nephritis 1.89
3 Acute pyelonephritis 1.77
4 Interstitial nephritis and acute pyelonephritis 0.73
5 Acute on chronic pyelonephritis 0.61
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.00
Secondary diagnoses and comments (if any):
Chronic renal damage too*7. Clinical info.*2. ANCA*1. ATN too*2. Drugs?*
18. Autoimmune screen*1. Gram stain*1. Renal imaging?*1.
Original report and further information (if any):
Acute interstitial nephritis, with some features raising the possibility of
ascending infection.
Circulation: W
Case number: 263
....
Number of responses:82 . Date of analysis: 19 JUL 06
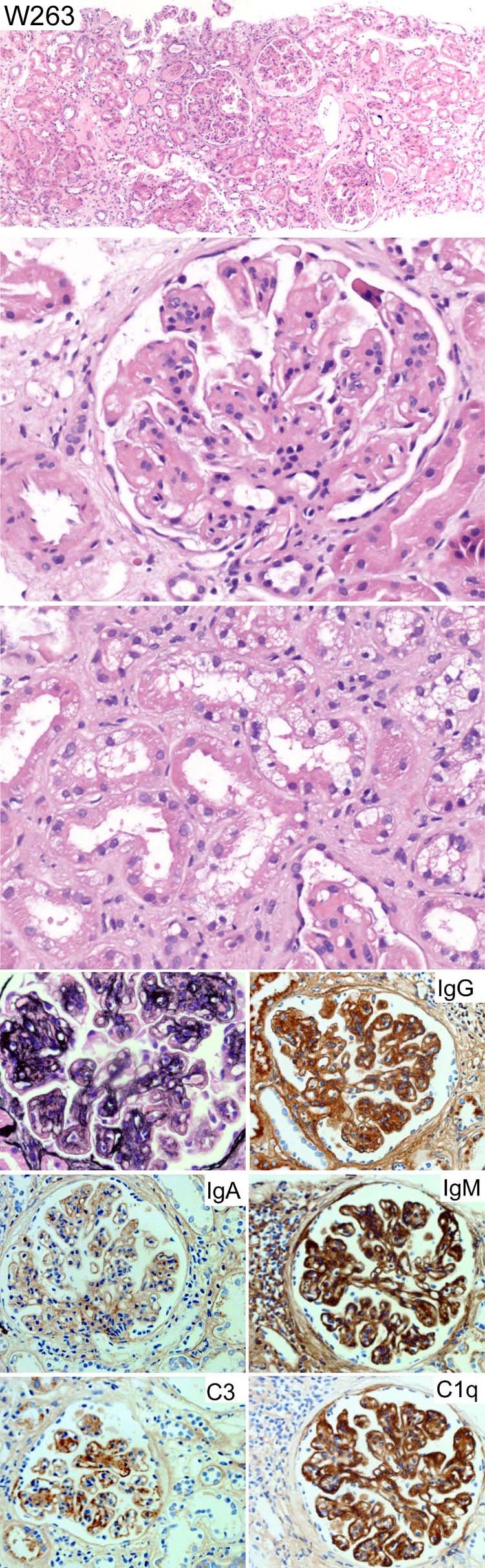
Clinical:
54 y.o male. History of hypertension. Painter and decorator. Proteinuria.
EM: Abundant large subendothelial amorphous electron dense deposits, in
places forming a continuous sausage-like appearance. No crystalline
deposits. Some mesangial deposits. No intramembranous or subepithelial
deposits. Widespread duplication of basement membrane. Capillary lumens
filled with mononuclear cells.
Specimen:
H&E, photos of Silver, IgA, IgM, IgG, C3 & C1q
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis 7.55
2 MCGn type II (dense deposit disease) 0.79
3 Membranoproliferative Gn - solvent nephropathy 0.12
4 SLE - class IV 1.41
5 Proliferative Gn, probably lupus IV G 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.55
Secondary diagnoses and comments (if any):
EM*10. PAS*1. MSB*1. Kappa & lambda immuno.*1. Exclude cryo*6. Various
causes of MCGn*6. Exclude lupus / lupus serology*31. C3 level?*2. C3nef?*1.
Congo red*1. Diabetes?*1. Hypertension *2. Repeat IgA*1. Exclude
leukaemia/lymphoma*1. Exposure to lead in paint?*1.
Original report and further information (if any):
Mesangiocapillary pattern, with immune complexes. K and L
immunohistochemistry inconclusive. Serum IgG kappa paraprotein 5.1g/l,
raised polyclonal IgM, cryo. repeatedly negative. No light chains in urine.
C3 low, C4 borderline low.
Circulation: W
Case number: 264
....
Number of responses:82 . Date of analysis: 19 JUL 06
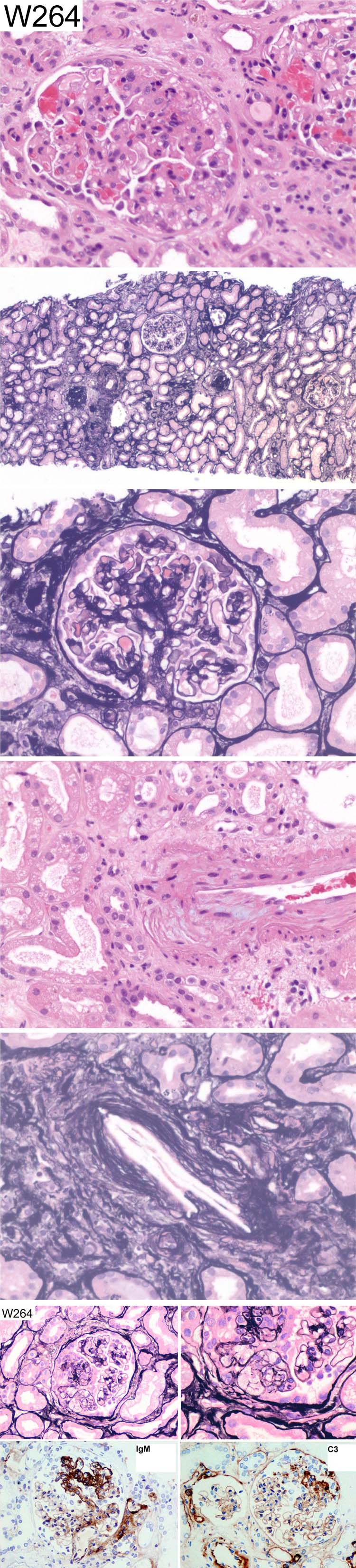
Clinical:
81 y.o male. Nephrotic (urine protein 24g per 24 hours). Creatinine has
risen from 100 to 300 in three weeks. MPO positive but low titre 4.8.
Active urine sediment with dysmorphic red cells. IgA and IgG negative.
Specimen:
H&E, Silver, Photos of IgM, C3 and Silver (x 2)
Diagnostic categories: Score:
1 FSGS (+/- collapsing) and cholesterol emboli 2.68
2 Primary FSGS (and variants) 5.29
3 Segmental proliferative Gn 0.30
4 Cholesterol emboli 0.24
5 Dense deposit disease 0.12
6 Scleroderma 0.06
7 Focal seg. necrotising Gn (+/-chol.emboli) 0.49
8 IgM nephropathy 0.32
9 Focal segmental proliferative/sclerosing Gn 0.37
10 Mesangial proliferative Gn and cholesterol emboli 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 5.29
Secondary diagnoses and comments (if any):
ATN too*6. Is FSGS due to atheroemboli?*3. Lesion on photos but not on
sections provided*2. Levels*1. EM*3. C1q*1. ANCA*1. ATN too*3. Underlying
diabetes?*3. Exclude endocarditis*1.
Original report and further information (if any):
Primary FSGS. (Cholesterol emboli not spotted on original sections)
Circulation: W
Case number: 265
....
Number of responses:81 . Date of analysis: 19 JUL 06
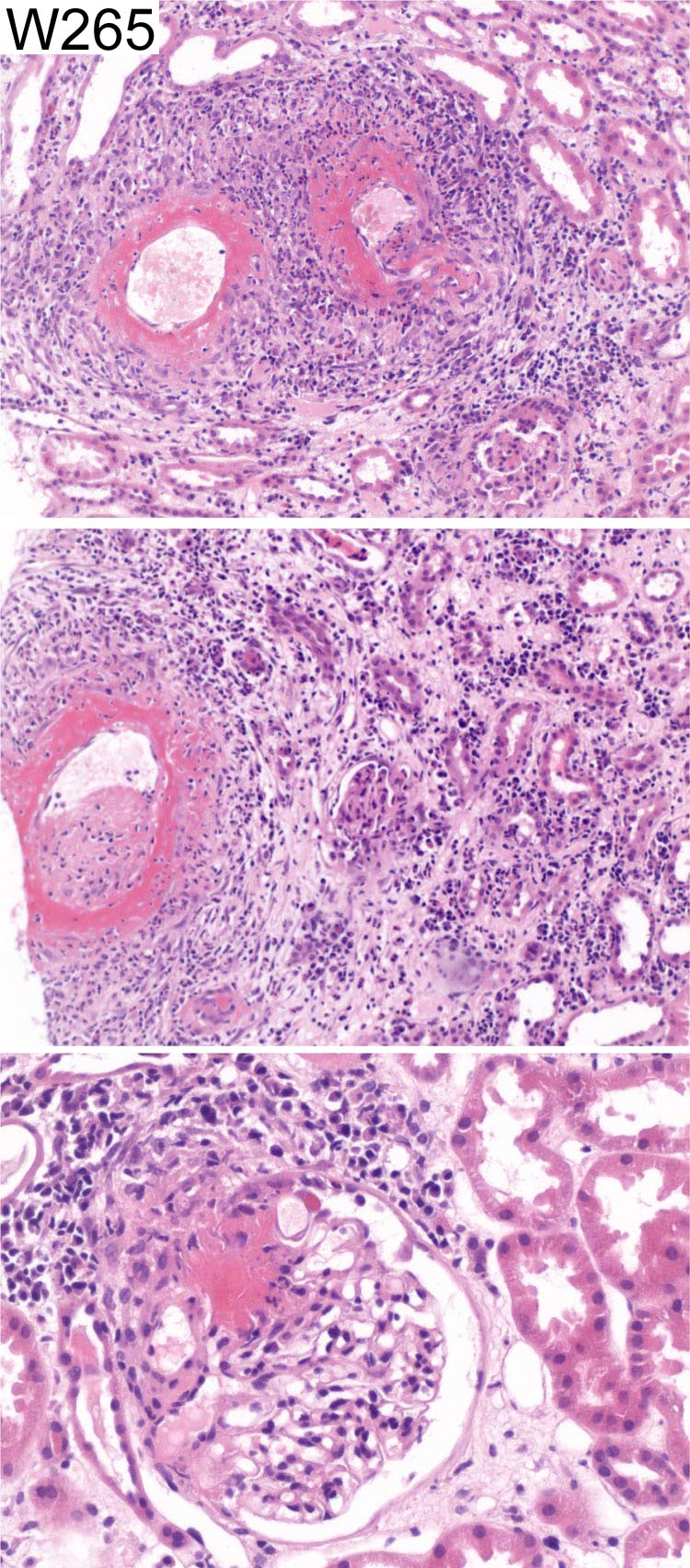
Clinical:
Female, 62 y.o. Fever and myalgia for one month. Raised temperature and
ESR/CRP. Blood and protein in urine. pANCA positive, MPO titre 119. Renal
function normal. Immunohistochemistry for IgG, IgA, IgM, C3 and C1q was
negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Microscopic polyangiitis 4.32
2 Pauci-immune vasculitis 3.70
3 Polyarteritis nodosa 1.85
4 Granulomatous vasculitis - Churg-Strauss 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.32
Secondary diagnoses and comments (if any):
Anti-GBM*1, Silver*1. PAS*1. Levels*1. More clinical info?*3.
Note from Organiser: Many different terms have been 'grouped' into
'microscopic polyangiitis'. We need to agree nomenclature here!
Original report and further information (if any):
ANCA small vessel vasculitis and glomerulonephritis
Links to cases in this document:
Top
W 260
W 261
W 262
W 263
W 264
W 265
Last updated: 19 JUL 06
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk