National Renal Pathology E.Q.A. Scheme
Circulation V
This document gives information on individual cases in
circulation V of this scheme. It contains no personal details
of participants.
Cases included:
V 254
V 255
V 256
V 257
V 258
V 259
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: V
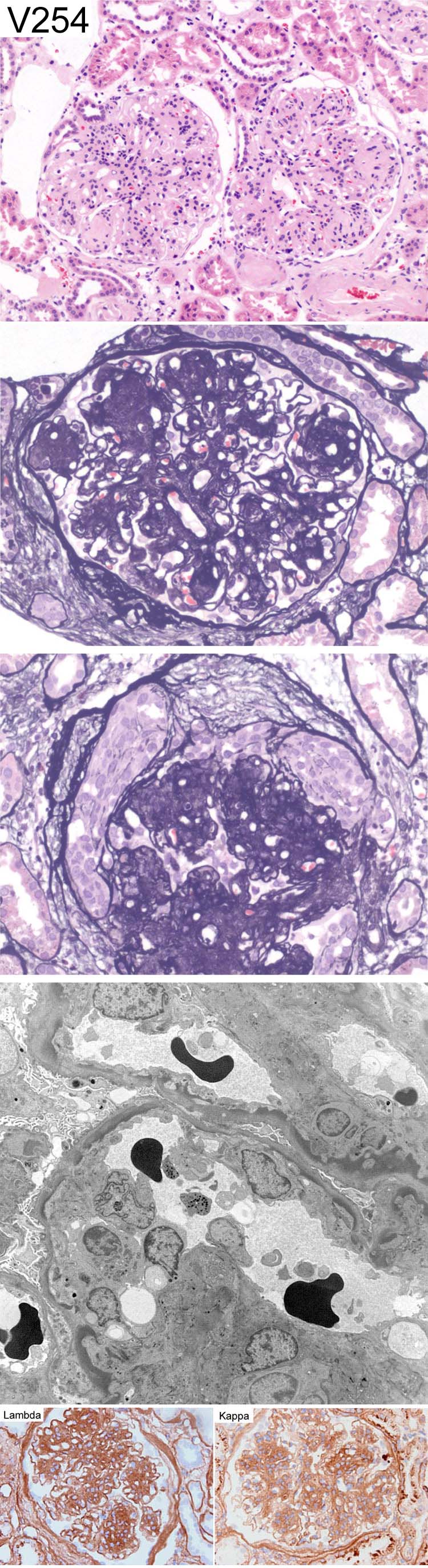
Case number: 254
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
50 y. o. male. End stage COPD and Nephrotic Syndrome. Proteinuria 4.9g/
24hr. Creatinine 121. ANA neg. C3 <0.78 and C4 <0.04. Plasma
electrophoresis IgG Lambda band. BJP present. Normal glucose tolerance.
U/S both kidneys 12.5cm. Congo Red negative. Immunoperoxidase: IF:
Mesangium and capillary wall IgG (traces). Light chain restriction is
equivocal for Lambda.
Specimen:
H&E, PAMS, Photos of EM, Kappa & Lambda
Diagnostic categories: Score:
1 Light chain nephropathy 7.37
2 Monoclonal immunoglobulin deposition disease 1.98
3 Cryoglobulinaemia (and light chain nephropathy) 0.12
4 Mesangiocapillary Gn 0.38
5 Diabetes 0.03
6 Not diagnostic (reaction to light chain deposits?) 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.37
Secondary diagnoses and comments (if any):
Immuno. for IgG subclasses*1. C3?*2. Atherosclerosis*1. ?diabetes*2.
PAS*2. BMT*2. IF*2. Repeat peroxidase*1. Higher mag. EM*6. EM of nodule*1.
Original report and further information (if any):
Light chain deposit disease (light chain nephropathy)
Circulation: V
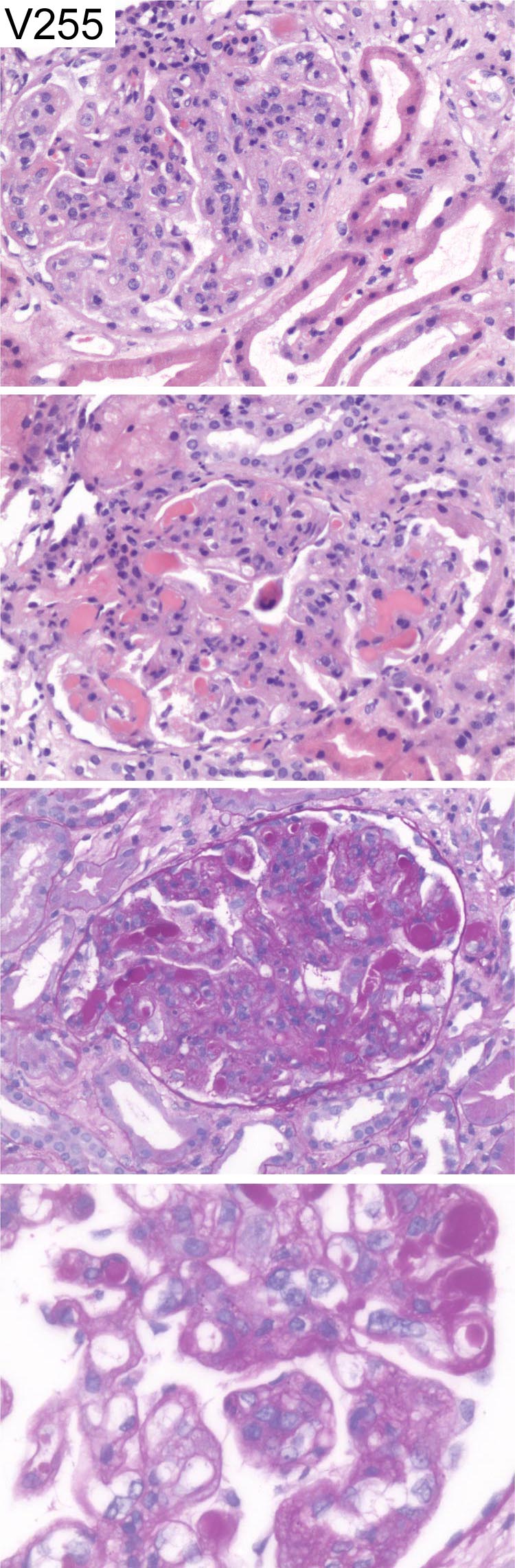
Case number: 255
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
60 year old female. Signs and symptoms of vasculitis, renal failure and
fluid overload. History of SLE/Sjogren's overlap syndrome. IF: Strong
mesangial and peripheral granular deposition of IgG, A, M and C3. The
hyaline intraluminal deposits strongly positive for all classes of
immunoglobulin and complement.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Lupus nephritis class IV (G, A) 4.19
2 Lupus nephritis class IV (G, A/C) 0.58
3 Lupus nephritis class IV (G) 0.35
4 Cryoglobulinaemia (exclude SLE) 0.35
5 Lupus nephritis class IV 2.23
6 Lupus nephritis class IV (S, A/C) 0.35
7 Cryoglonulinaemia 0.67
8 Cryoglobulinaemia (due to MCTD or lupus?) 0.12
9 Lupus nephritis NOS 0.47
10 MCGn 2ry to ?lupus ?cryo 0.70
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.19
Secondary diagnoses and comments (if any):
EM*10. Exclude cryoglobulins*17. Antiphospholipid?*3. C1q?*4. Lupus
serology*1. Silver stain *4. MSB*1. C;linical evidence of lupus?*2.
Original report and further information (if any):
Diffuse (class 4) lupus glomerulonephritis with focal activity
Circulation: V
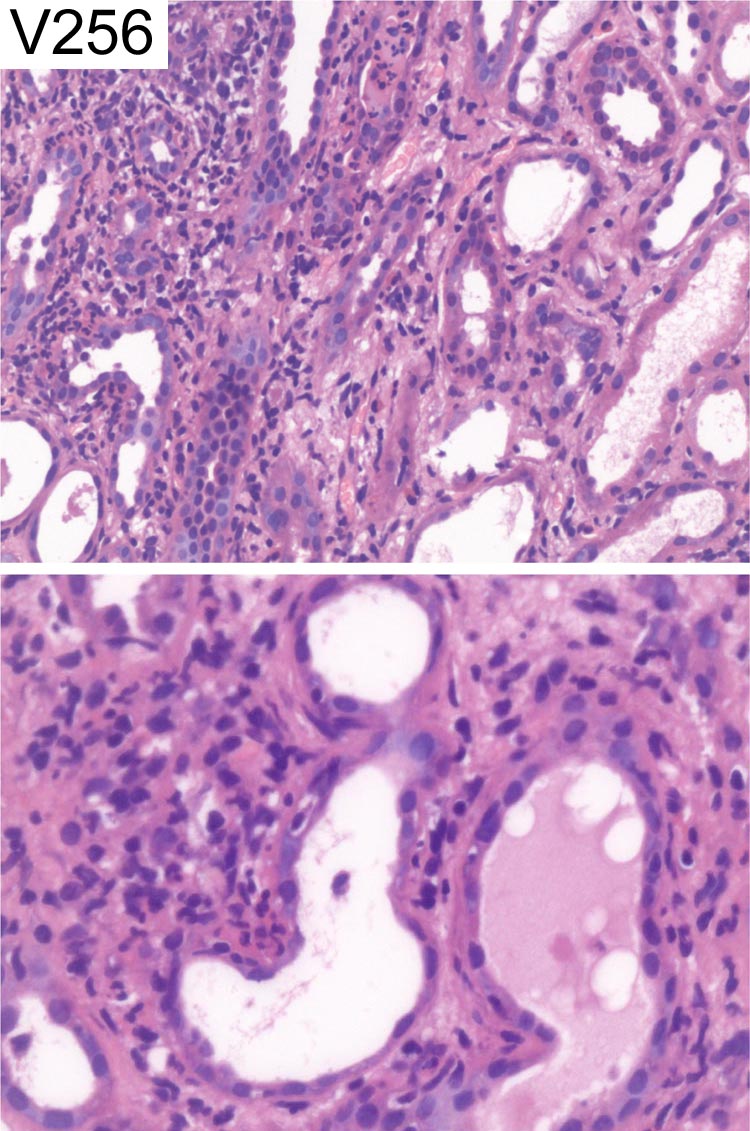
Case number: 256
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
62 y.o. female. Acute renal failure. Positive urinary sediment. No
previous clinical history of note. ANCA negative. Recent E. coli urinary
tract infection treated with antibiotics.
Specimen:
H&E
Diagnostic categories: Score:
1 Tubulointerstitial nephritis and ATN 0.58
2 Tubulointerstitial nephritis 6.73
3 Acute pyelonephritis (consider TIN) 0.23
4 Acute pyelonephritis 1.29
5 Interstitial nephritis and acute pyelonephritis 1.05
6 Interstitial nephritis and residual pyelonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.73
Secondary diagnoses and comments (if any):
Exclude residual infection*22. PAS*3. Gram*1. Grocott*1. Drug related /
allergic?*31. Also HUS/TTP?*1. Also ATN*1. Immunohistochemistry*1. Blood
cultures*1. What's a 'positive sediment'?*1.
Original report and further information (if any):
Tubulo-interstitial nephritis
Circulation: V
Case number: 257
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
57 y.o. male. History of pancreatitis and NIDDM with retinopathy. Low
grade proteinuria (0.6 g/l) and creatinine of 240. Immunostaining showed a
few flecks of IgM and larger amounts of C1q in a mesangial pattern and in
blood vessels. Congo Red stain negative.
Specimen:
H&E, PAS & Photo's of EM x 2
Diagnostic categories: Score:
1 Diabetic nephropathy 9.41
2 FSGS 0.20
3 C1q nephropathy 0.16
4 Diabetic retinopathy (that's what it said!) 0.12
5 Mesangial hyperplasia, not diabetic nephropathy 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.41
Secondary diagnoses and comments (if any):
Scale on EM / GBM thickness*3. ATN too*3. C1q nephropathy?*4. More EM*1.
Silver*1. Congo red*1. Complaints about pale H&E.
Original report and further information (if any):
Diabetic nephropathy; exclude renal vein thrombosis.
Circulation: V
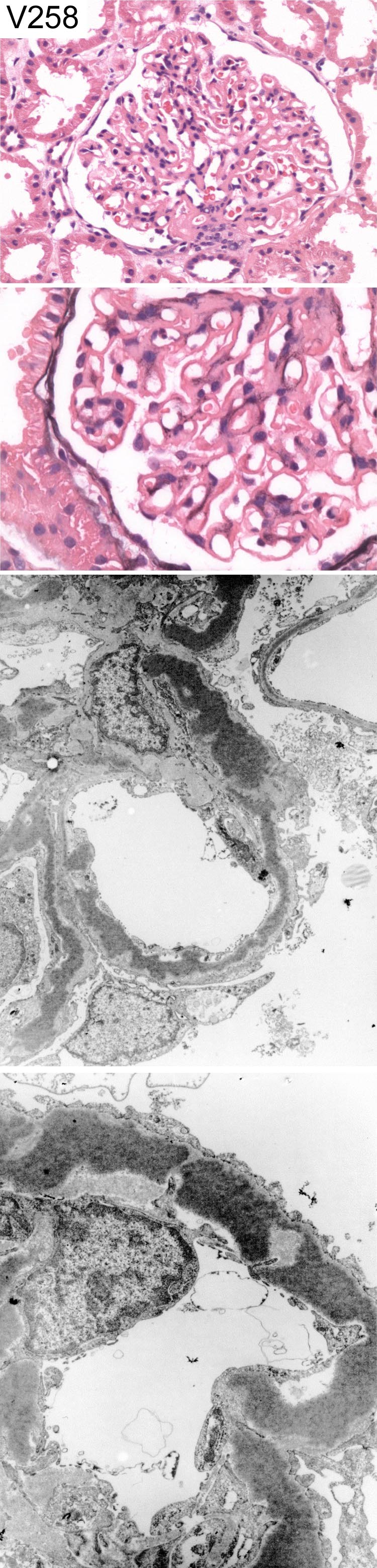
Case number: 258
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
24 y.o. female. Six months post partum. proteinuria 4+. Haematuria +.
Uneventful pregnancy. Normotensive. Normal renal function. Negative
immunology. No past history of renal disease. Immunohistochemistry -
linear basement membrane and mesangial staining for C9 and IgM to lesser
extent. IgA and IgG negative.
Specimen:
H&E, PAMS, Photos of EM x 2
Diagnostic categories: Score:
1 Dense deposit disease (MCGn type II) 8.95
2 Toxaemia of pregnancy 0.23
3 MCGn type I 0.12
4 Membranous Gn 0.35
5 Cryoglobulinaemia (MPGn pattern) 0.12
6 Difuse proliferative Gn ? lupus 0.12
10 No diagnosis. Check ANA, redo IHC 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.95
Secondary diagnoses and comments (if any):
C3?*6. C3Nef?*3.Serum complement levels?*2. Exclude endocarditis*1.
Partial lipodystrophy?*1. Better silver stain*6. PAS*1. Should 'C9' read
'C3'?*3. Hepatitis serology?*2. Congo red*1. Should be education only*1.
Original report and further information (if any):
Circulation: V
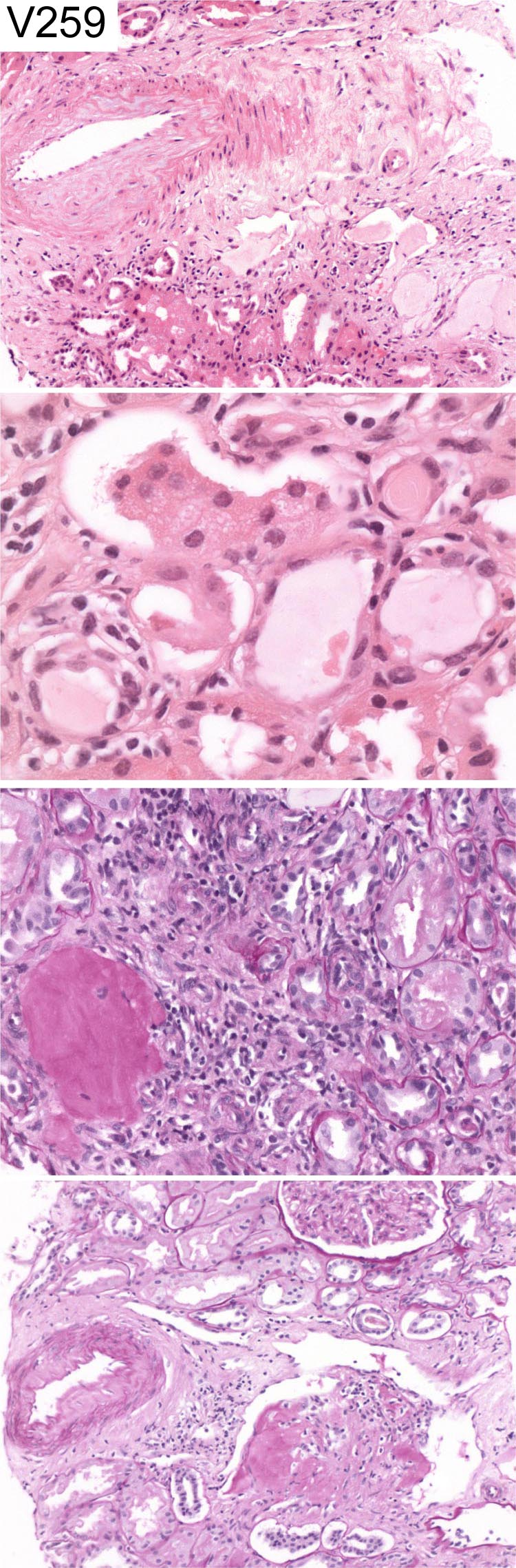
Case number: 259
....
Number of responses:86 . Date of analysis: 19 JUL 06
Clinical:
54 y.o. male. Creatinine 300. Unwell. Non-specific atypical kappa
paraprotein band. ?Myeloma. No past history. BP 130/80. IF : Significant
immune deposits present within glomeruli. Several casts reactive for kappa
but negative for lambda.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Myeloma cast nephropathy 8.20
2 Amyloidosis 0.06
3 Light chain deposition disease 0.51
4 Light chain glomerulopathy and cast nephropathy 0.23
5 Interstitial nephritis 0.12
6 Light chain cast nephropathy (???) 0.12
7 Acute tubular necrosis 0.07
10 Inadequate, no diagnosis 0.70
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.20
Secondary diagnoses and comments (if any):
Congo red*8. Inadequate / not suitable for EQA*41. EM*6. IF*1. Urine
light chains?*3. BM*2. What does 'significant immune deposits' mean?*19
(I've no idea, ask the submitting pathologist - PF)
Original report and further information (if any):
Light chain cast nephropathy (kappa paraprotein). No evidence of amyloid.
Links to cases in this document:
Top
V 254
V 255
V 256
V 257
V 258
V 259
Last updated: 19 JUL 06
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk