National Renal Pathology E.Q.A. Scheme
Circulation T
This document gives information on individual cases in
circulation T of this scheme. It contains no personal details
of participants.
Cases included:
T 242
T 243
T 244
T 245
T 246
T 247
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: T
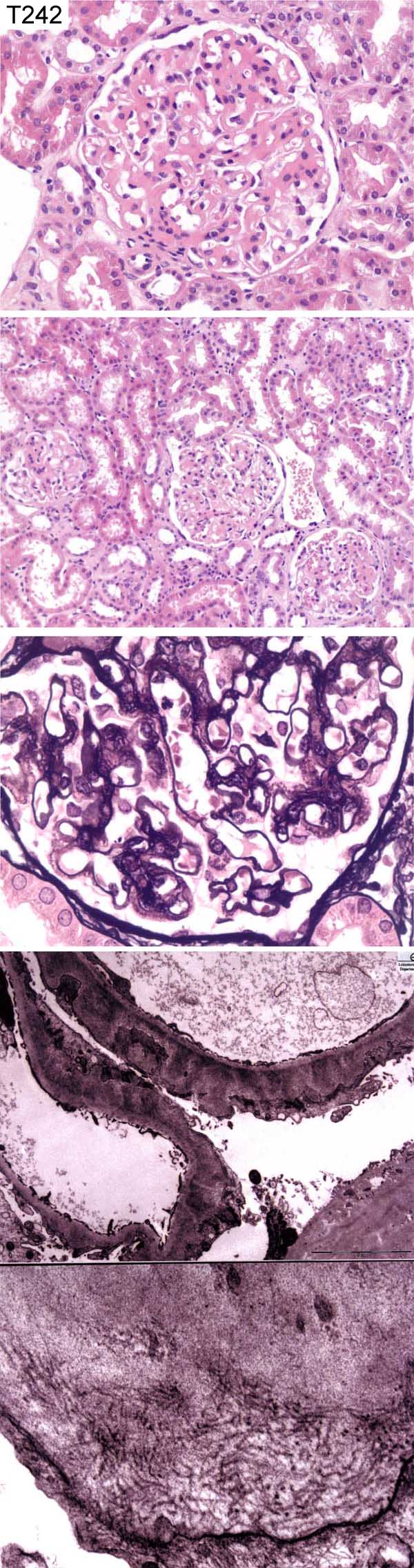
Case number: 242
....
Number of responses:83 . Date of analysis: 31 DEC 05
Clinical:
38 year old female. Increased cholesterol, overweight, nephrotic range
proteinuria. Congo Red negative. ICC - fine granular IgG and C3 on GBM;
IgM and IgA negative.
Specimen:
H&E, Meth Ag, Photos of EM *2
Macro:
For education and interest only
Diagnostic categories: Score:
1 Membranous Gn 1.06
2 Memb. Gn with 'structured' deposits 0.52
3 Fibrillary Gn, membranous pattern 1.27
4 Fibrillary Gn 4.46
5 Immunotactoid Gn 1.27
6 Amyloid 0.16
7 Membranous AND amyloid 0.48
8 Non-amyloid structured deposits 0.60
9 Membranous amyloid 0.12
10 Light chain nephropathy 0.06
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 4 with 4.46
Secondary diagnoses and comments (if any):
EM of mesangium*4. Scale / Fibril size*10. Repeat Congo red*5. Diabetes?*1.
Exclude plasma cell monoclonality*4. Exclude cryo.*1. SLE serology*2.
Complement levels?*1. Collagen III immunostaining*1.
Original report and further information (if any):
Circulation: T
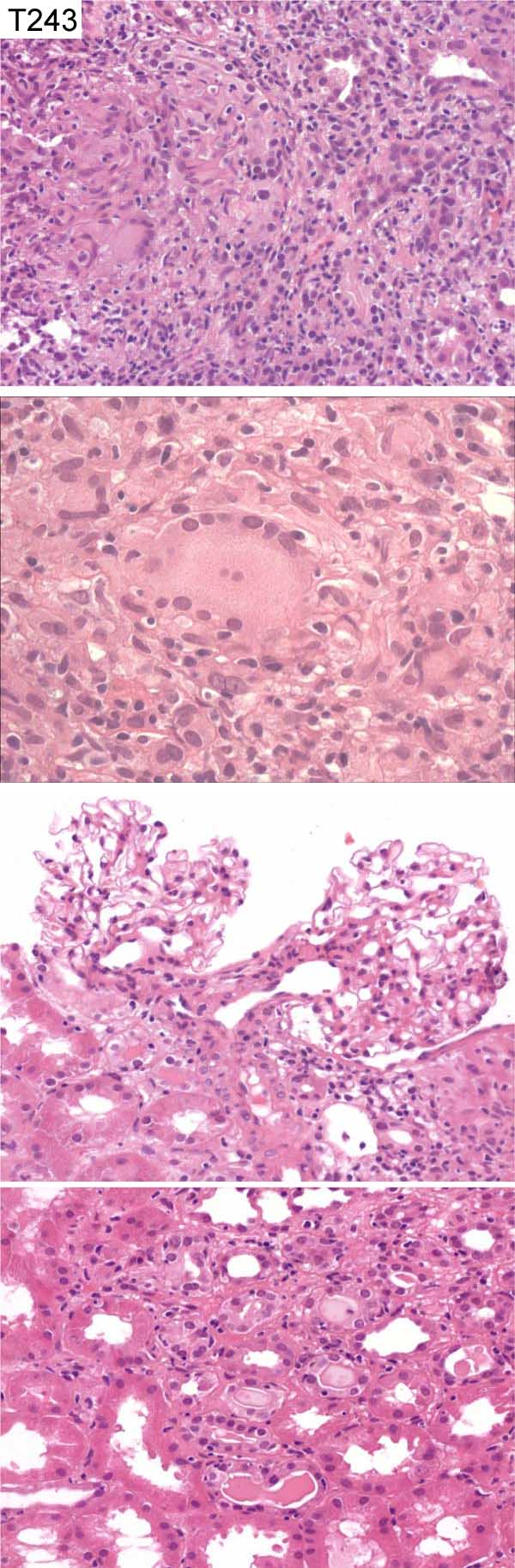
Case number: 243
....
Number of responses:83 . Date of analysis: 31 DEC 05
Clinical:
Unexplained rapid deterioration in renal function. Mild proteinuria. ?
RPGN. ?Myeloma. ?Infiltrative process. Staining for AAFBs was negative.
IF negative and EM showed no specific glomerular abnormality.
Specimen:
H&E
Diagnostic categories: Score:
1 Granumomatous interstitial nephritis ?sarcoid 1.55
2 Sarcoid 0.00
3 Granulomatous interstitial nephritis, differential given5.54
4 Granulomatous interstitial nephritis NOS 2.65
5 Interstitial nephritis 0.00
6 Granulomatous nephritis, ?TB 0.13
7 Granulomatous nephritis ?drug reaction 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 5.54
Secondary diagnoses and comments (if any):
Age, sex?*3. Ethnic origin?*1. More clinical info.*5. Stains for other
organisms/exclude infection*12. PCR for mycobacteria*1. ?drugs*5. Serum
ACE*5. ANCA*7. CXR*5. Serum Ca*1. Exclude myeloma*3.
Original report and further information (if any):
Granulomatous interstitial nephritis. No evidence of TB or drugs. ACE
raised at time of biopsy; interpreted clinically as 'renal sarcoid' but no
extra-renal sarcoid. ACE then normalised. Treated with prednisolone;
function returned to normal and remained so.
Circulation: T
Case number: 244
....
Number of responses:83 . Date of analysis: 31 DEC 05
Clinical:
Female, 23 y.o. Mild proteinuria and haematuria. Immunoperoxidase staining
showed mesangial IgM+ but no glomerular localisation of IgA, IgG, C1q, C3 or
C4.
Specimen:
H&E, EM x 5
Diagnostic categories: Score:
1 Hereditary nephropathy, Alport type 6.90
2 Hereditary nephropathy NOS 0.36
3 IgM nephropathy 0.60
4 FSGS 1.17
5 Thin membrane nephropathy 0.36
6 Hereditary nephropathy - Nail patella syndrome? 0.12
7 Minimal change 0.24
8 Heterozygous Fabry's disease 0.12
10 No diagnosis offered 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.90
Secondary diagnoses and comments (if any):
Autosomal type Alport*5. EM prints too pale *6. Silver stain*1. Lipid
stain*1. Family history?*21. Clinical / extra-renal manifestations?*6.
Type IV col. alpha chain immuno*11. Confirmation by genetics*3. Exclude
diabetes*1.
Original report and further information (if any):
Circulation: T
Case number: 245
....
Number of responses:83 . Date of analysis: 31 DEC 05
Clinical:
59 y.o. Male. Rapidly progressive acute renal failure. Creatinine 540
umol. Nephrotic with ascites, peripheral oedema, hypo-albuminaemia and
proteinuria. On clinical examination he had a purpuric rash on the buttocks
and feet. Auto-antibody screen, ANCA and anti GBM results not available.
Specimen:
H&E, PAS, Meth Ag. Photos IgA
Diagnostic categories: Score:
1 HSP / IgA nephropathy 9.47
2 HIV nephropathy 0.12
3 Lupus 0.07
4 Cryoglobylinaemia 0.02
5 Acute proliferative glomerulonephritis 0.22
6 Collapsing glomerulopathy 0.03
7 Post-infectious Gn 0.06
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.47
Secondary diagnoses and comments (if any):
EM*13. Rest of IF?*14. ATN too*7. Also thrombotic microangiopathy*1. Also
interstitial nephritis*1. Lupus serology*4. IgA nephr. in HIV infection?*1.
ASOT*1. Not suitable for EQA*1.
Original report and further information (if any):
Henoch Schonlein purpura. No follow-up info.
Circulation: T
Case number: 246
....
Number of responses:83 . Date of analysis: 31 DEC 05
Clinical:
Male, 15 y.o. Presented with nephrotic syndrome two weeks previously.
Rising creatinine. Positive ANA and decreased complement lelves. ?Lupus.
There is strong staining for all immunoreactants throughout loops and
mesangium.
Specimen:
H&E, MAg, Photos of EM x 2 and IF
Diagnostic categories: Score:
1 Lupus class IV (G, A) 6.12
2 Lupus class IV (A) 0.72
3 Lupus nephritis NOS 0.60
4 Lupus IV NOS 2.23
5 Post-infective Gn 0.01
6 MPGN / MCGN 0.07
7 MPGN pattern, could be lupus 0.12
8 Lupus IV (G, A/C) 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.12
Secondary diagnoses and comments (if any):
Lupus serology?*6. EM*1. Clinical evidence of lupus?*1. Antiphospholipid
Abs?*1. Exclude cryo.*2. HBV?*1. Inadequate info, ?suitable for EQA*1.
Original report and further information (if any):
Lupus nephritis, WHO class IV-G
Circulation: T
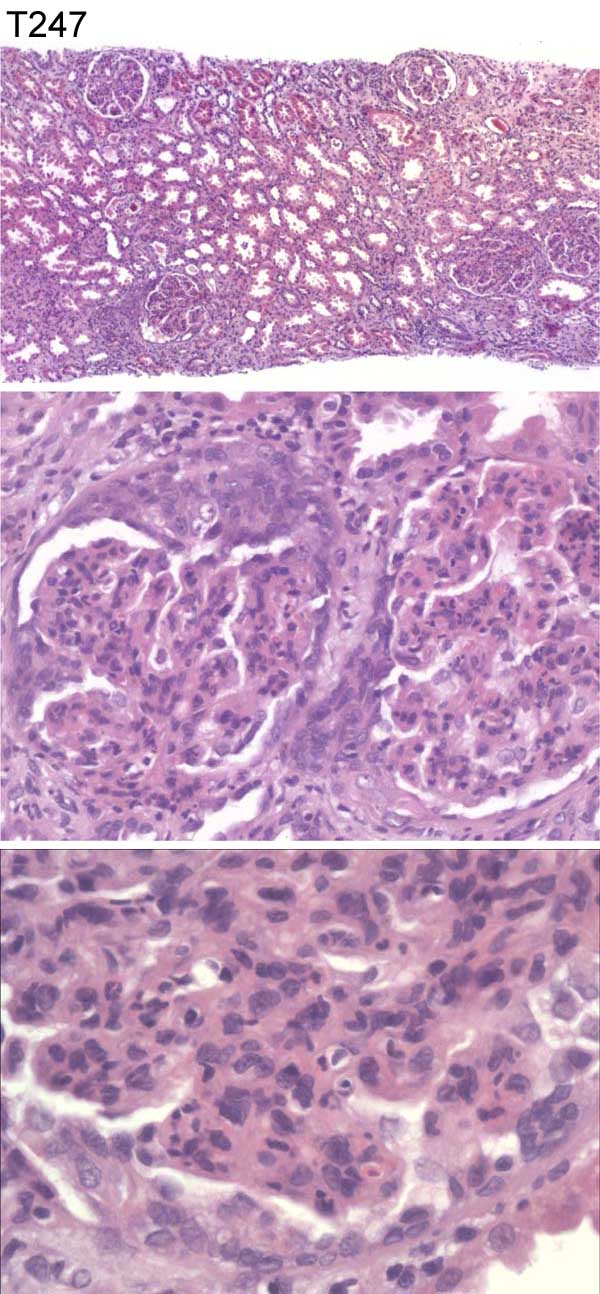
Case number: 247
....
Number of responses:82 . Date of analysis: 31 DEC 05
Clinical:
47 year old female. Recent S.A.H. clipping and post-op staph sepsis.
Developed nephrotic syndrome with poor urine output despite diuretics. All
immunology negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Proliferative endocap./post-infective Gn 8.73
2 Mesangiocapillary Gn post infection 0.17
3 Diffuse prolif Gn ? cause 0.49
4 Endocapillary Gn AND interstitial nephritis 0.12
5 Pauci-immune crescentic Gn 0.24
6 Mesangiocapillary glomerulonephritis 0.12
10 No diagnosis offered 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.73
Secondary diagnoses and comments (if any):
IF*21. Does 'immunology negative' mean serology or IF?*10. Why is IF
negative?*5. EM*25. Silver stain *12. PAS*1. Trichrome*1. Adequate for
EQA with only H&E?*5. ASOT*2. ANCA*1. Hypertension too*1. Interstitial
nephritis too?drugs*2. Acute pyelo too?*1. Serum C3?*1.
Original report and further information (if any):
Acute proliferative glomerulonephritis, in keeping with post-infectious
glomerulonephritis
Links to cases in this document:
Top
T 242
T 243
T 244
T 245
T 246
T 247
Last updated: 31 DEC 05
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk