National Renal Pathology E.Q.A. Scheme
Circulation R
This document gives information on individual cases in
circulation R of this scheme. It contains no personal details
of participants.
Cases included:
R 230
R 231
R 232
R 233
R 234
R 235
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: R
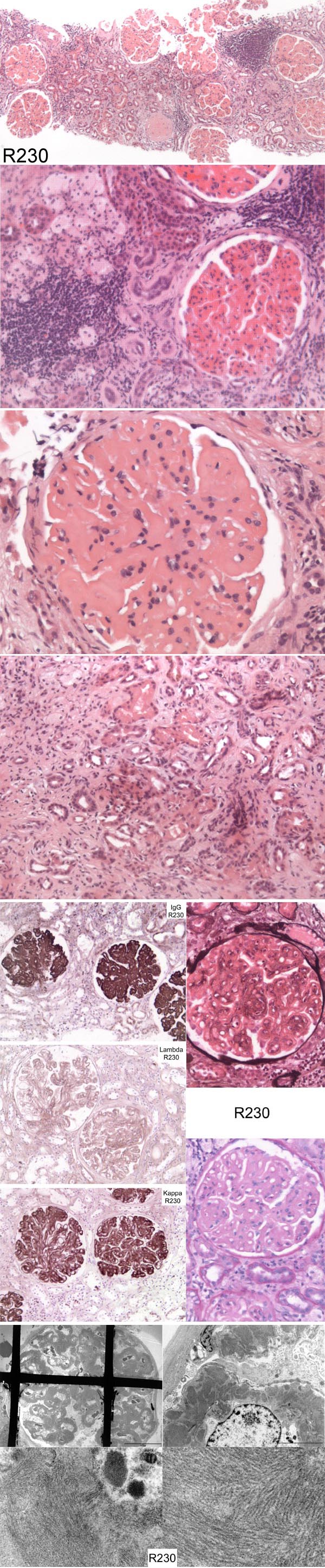
Case number: 230
....
Number of responses:79 . Date of analysis: 24 APR 05
Clinical:
69 y.o female presented with nephrotic range proteinuria and impaired renal
function. No serological or clinical evidence of lupus. Subsequently found
to have CLL. Congo red negative. Fibril diameter measured (on second
attempt!) at 'about 20nm'.
Specimen:
H&E. Photos of IPx,, EM, PAS and Silver
Diagnostic categories: Score:
1 Fibrillary Gn 5.41
2 Fibrillary Gn secondary to lymphoid neoplasia 0.13
3 Fibrillary / immunotactoid glomerulopathy 1.01
4 Fibrillary Gn due to light chain deposition 0.13
5 Immunotactoid glomerulopathy 1.84
6 Non-amyloid monoclonal Ig deposition disease 0.85
7 Light chain deposition disease 0.32
8 Atypical membranous Gn 0.05
9 MPGn/cryoglobulin 0.22
10 Amyloid 0.06
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.41
Secondary diagnoses and comments (if any):
Exclude lymphomatous infiltration*8. Secondary to CLL?*6.
Immunoelectrophoresis*6. Cryoglobulins?*11. IPx for IgM?*1. Sponge/mesh
artefact*1. Better EM*2. Repeat Congo red*2. Exclude HIV*1. Unsuitable
for EQA*1.
Original report and further information (if any):
Circulation: R
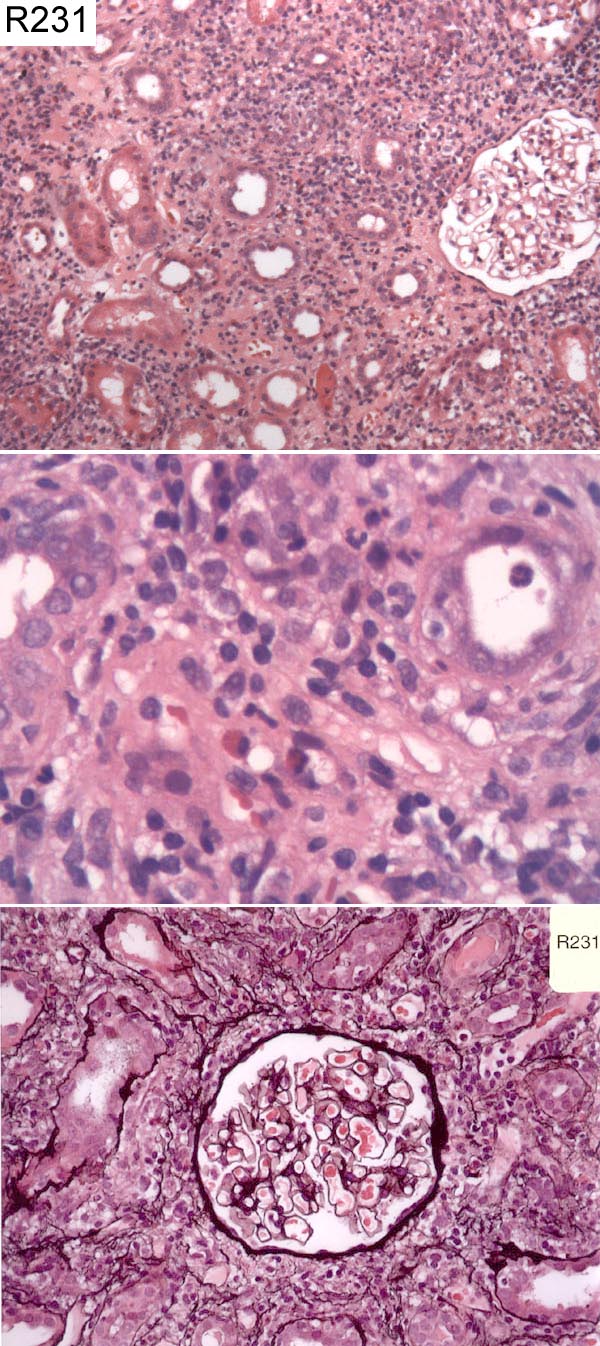
Case number: 231
....
Number of responses:79 . Date of analysis: 24 APR 05
Clinical:
Male 22 y.o. History of cough five weeks previously. Creatinine now 260.
Blood and protein in urine. Abnormal clotting and lupus coagulant.
Strongly positive Anti-streptolysin (ASO) titre (1/1600). Recently treated
with Erythromycin and Ibuprofen, for cough and headache respectively.
Specimen:
H&E, Photo of Meth. Silver
Diagnostic categories: Score:
1 Acute tubulo-interstitial nephritis 9.80
2 Haemolytic uraemic sundrome 0.06
3 Interstitial nephritis +/- thrombotic microangiopathy 0.13
4 Acute pyelonephritis 0.01
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.80
Secondary diagnoses and comments (if any):
Presumably secondary to drugs*35. Infection?*8. Lupus?*3. IF*5. EM*4.
Insufficient material for EQA*1.
Original report and further information (if any):
Circulation: R
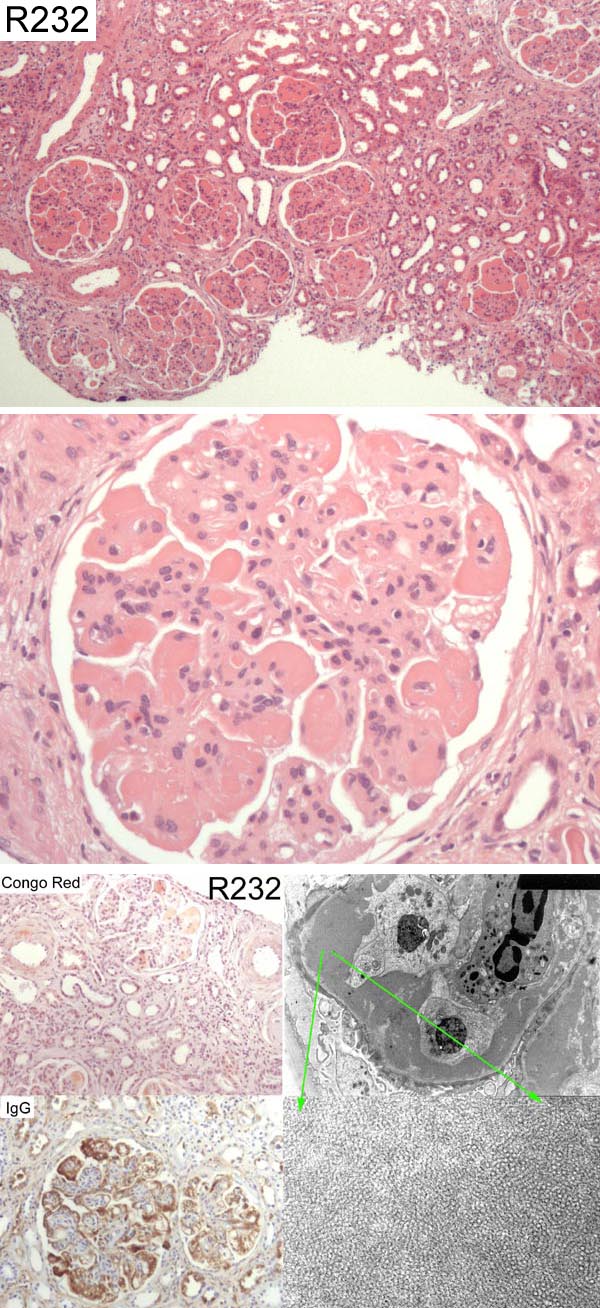
Case number: 232
....
Number of responses:79 . Date of analysis: 24 APR 05
Clinical:
58 y.o male. Normal serum creatinine January 1999, up to 153 on 4/2000.
Monoclonal gammopathy of uncertain significance diagnosed June 1999. IHD,
CABG, AVR, HTN, referred September 01 with creatinine up to 229. Urinalysis
blood and protein, albumin 29, Free Lambda light chains in urine. Rectal
biopsy negative for amyloid. Congo Red - as photo but NO dichroism under
polaroids. IPX: IgA, M and C3 like IgG.
Specimen:
H&E, Silver, Photos of EM, IgG, Congo Red
Diagnostic categories: Score:
1 Immunotactoid glomerulonephritis 3.97
2 Cryoglobulinaemia 2.04
3 Mesangiocapillary Gn (secondary to cryo?) 0.78
4 Light chain nephropathy 1.37
5 Non-amyloid organised deposit disease 0.44
6 Amyloid 0.05
7 Monoclonal immunoglobulin deposition disease 0.84
8 Lupus 0.20
9 Fibrillary Gn 0.30
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 3.97
Secondary diagnoses and comments (if any):
Clinical evidence of cryoglobulinaemia?*1. Serum cryo?*16. Serum
complement?*1. Hepatitis status?*2. Lupus serology*6. Measurements of
fibril size/EM magnification?*11. Exclude diabetes*1. Repeat Congo Red*1.
IF for K&L*5. Unsuitable for EQA*1.
Original report and further information (if any):
Immunotactoid glomeruopathy.
Circulation: R
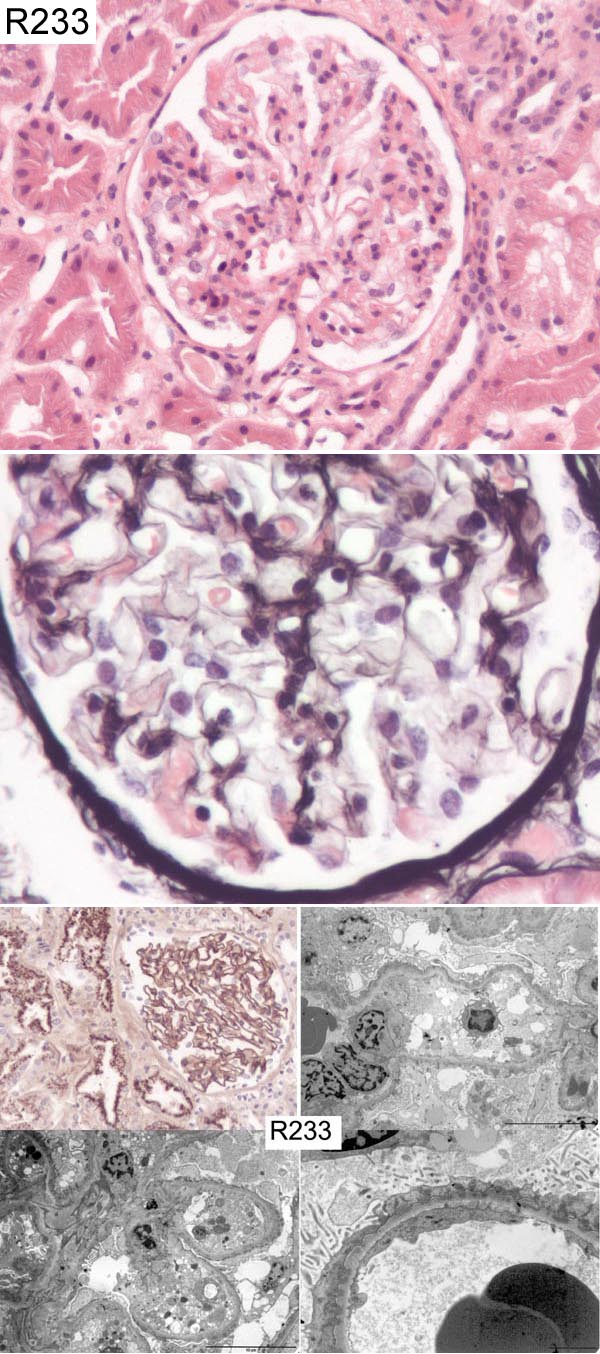
Case number: 233
....
Number of responses:79 . Date of analysis: 24 APR 05
Clinical:
51 y.o. male. Nephrotic syndrome. Immunofluorescence showed strong
staining for IgG in a granular pattern around capillary basement membranes
and less strong staining for complement. IgA and IgM were negative. EM
showed dense deposits in a subepithelial location.
Specimen:
H&E, Silver, Photos of IgG and EM
Diagnostic categories: Score:
1 Membranous Gn 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Rectal examination.*1. (I did NOT make that up! - PF)
Original report and further information (if any):
Membranous glomerulonephritis despite suspiciously 'linear' IgG
Circulation: R
Case number: 234
....
Number of responses:79 . Date of analysis: 24 APR 05
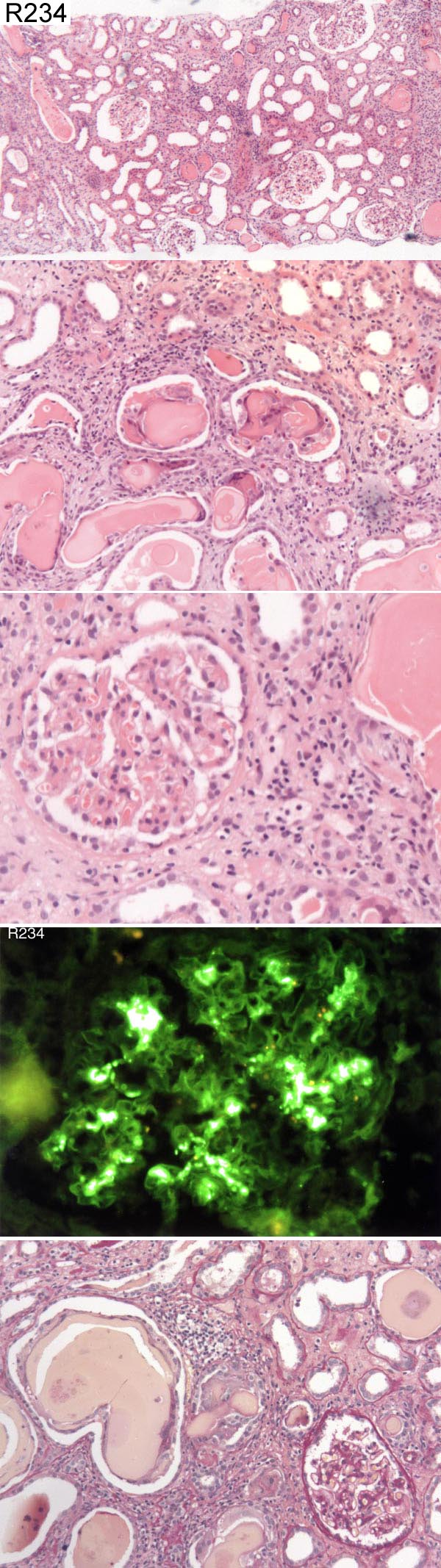
Clinical:
45 y.o. male. Presenting with acute renal failure. 4 mth history of chest
wall pain. Had been taking non-steroidal anti-inflammatories for past 6
weeks. Serum biochemistry demonstrated high calcium and elevated alkaline
phosphatase. He was also found to be anaemic. IF staining was negative for
IgG and IgM. C3 showed the same as IgA (see photo).
Specimen:
H&E, PAS (but actually a van Gieson?) Photo of IF (IgA)
Diagnostic categories: Score:
1 Myeloma cast nephropathy 3.42
2 Myeloma cast nephropathy and IgA nephropathy 6.08
3 Light chain cast nephropathy and IgA nephropathy 0.13
4 Tubulointerstitial nephritis & IgAN 0.13
5 IgA myeloma 0.25
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.08
Secondary diagnoses and comments (if any):
Investigations to confirm myeloma*12. Presence of haematuria?*1. IgA
nephropathy is presumably incidental*7. Exclude IgA myeloma?*3. Exclude
infection*1. EM*10. Congo red*3. TIN too*2. ATN too*1. Kappa and
lambda*3.
(PAS is an 'Oxford PAS', not a VG - *1)
Original report and further information (if any):
Circulation: R
Case number: 235
....
Number of responses:78 . Date of analysis: 24 APR 05
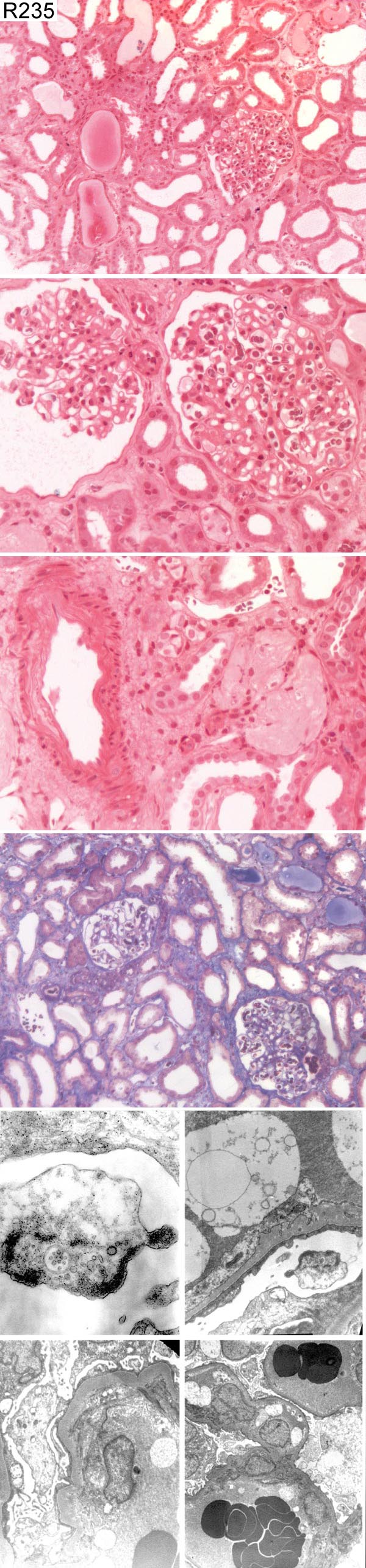
Clinical:
60 y.o male. HIV+ more than 10 years but still very low viral load. He is
nephrotic, creatinine levels rose acutely to 320 with marked proteinuria.
Signs of tubular necrosis were attributed to drug reaction; clinically
expected since his medication had been changed.
Specimen:
H&E, AFOG, Photos of EM
Macro:
Lack of haematoxylin and small EM images noted by Organiser. Don't shoot the
messenger! - PF
Diagnostic categories: Score:
1 HIV nephropathy 5.06
2 FSGS/minimal change spectrum 1.86
3 Membranous Gn 0.13
4 FSGS 0.32
5 Collapsing glomerulopathy 0.13
6 Acute tubular necrosis 0.71
7 Infection 0.32
8 Sickling disorder 0.26
9 Mesangiocap. / membranoprolif. Gn 0.26
10 Refused to offer diagnosis 0.96
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.06
Secondary diagnoses and comments (if any):
IF*7. ATN too*6. HUS too?*1. ZN*1. Gram*1. CMV?*2. Polyoma?*1. Exclude
renal vein thrombosis*1. Giemsa*1. PAS*1. EM*2.
What's an AFOG?*4. Poor sections*7. Poor photos*8. Not suitable for
EQA*21. Shoot the submitting pathologist then!*1.
Original report and further information (if any):
Minimal change nephropathy, which proved steroid sensitive. Evidence of ATN
attributed to a drug reaction (medication had been changed).
Links to cases in this document:
Top
R 230
R 231
R 232
R 233
R 234
R 235
Last updated: 24 APR 05
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk