National Renal Pathology E.Q.A. Scheme
Circulation P
This document gives information on individual cases in
circulation P of this scheme. It contains no personal details
of participants.
Cases included:
P 218
P 219
P 220
P 221
P 222
P 223
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: P
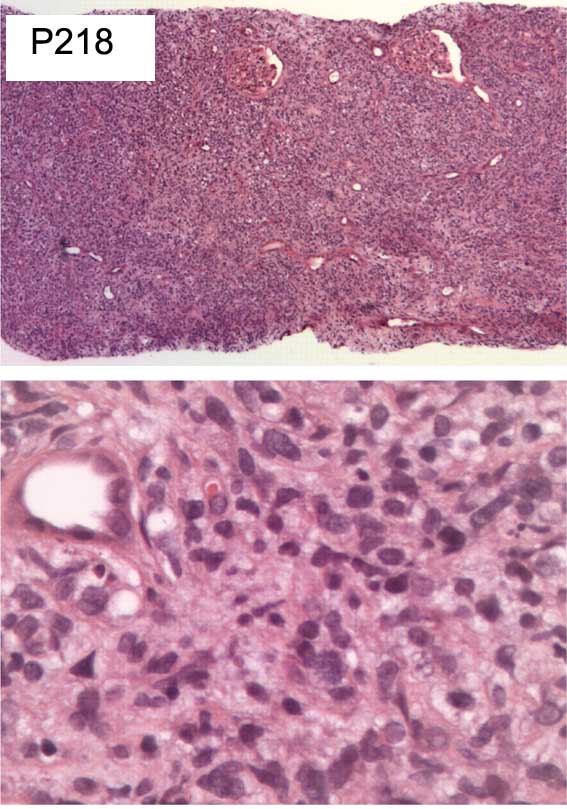
Case number: 218
....
Number of responses:79 . Date of analysis: 14 AUG 04
Clinical:
Male, 46 yrs old. Previous history of cutaneous lymphoma diagnosed four (4)
years ago. Acute renal failure with fever and enlarged kidneys.
Specimen:
H&E
Diagnostic categories: Score:
1 Lymphoma NOS 7.20
2 High grade lymphoma 1.39
3 Probable lymphoma, do studies to confirm 1.14
4 Granulomatous inflam, exclude TB if not monoclonal 0.01
5 Sarcomatoid carcinoma, do immuno. 0.13
6 Malignat tumour, do immuno. 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.20
Secondary diagnoses and comments (if any):
Lymphoma immuno.*50. Specialist lymphoma opinion*3. Review cutaneous
lymphoma*16
Original report and further information (if any):
Circulation: P
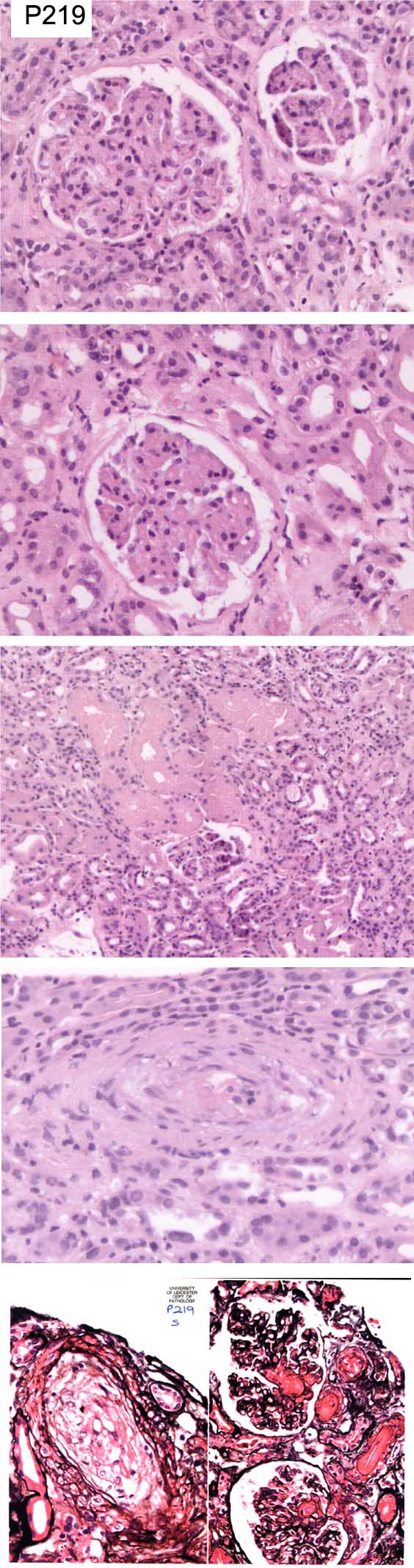
Case number: 219
....
Number of responses:79 . Date of analysis: 14 AUG 04
Clinical:
Female, 70 yrs old. Presented with acute renal failure. H/O Raynaud's
syndrome and skin changes ?connective tissue disorder. ANA positive.
Rheumatoid factor positive, double stranded DNA antibodies negative. Other
auto-antibodies pending. Blood pressure mildly elevated. Platelets normal.
Immunofluorescence showed no evidence of glomerular deposition of IgG, IgM,
IgA, C3 or C4.
Specimen:
H&E, photos of Silver *2
Diagnostic categories: Score:
1 Thrombotic microangiopathy, cause not suggested 0.13
2 Microangiopathy ? systemic sclerosis 8.72
3 Microangioathy, differential given 0.76
4 Microangiopathy ? connective tissue disorder 0.13
5 Cryoglobulinaemia 0.01
6 Mixed connective tissue disease 0.13
7 Mucoid vasculopathy and ischaemia 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 8.72
Secondary diagnoses and comments (if any):
Need section stained for vessels*1. Alcian blue*1. Need clinical info.*6.
Anti-RNP serology*5. ANCA?*1. Calcium level?*1. Haematological evidence of
HUS/TTP?*8. Poor photos*2. EVG*2. MSB*1.
Original report and further information (if any):
Final clinical diagnosis: Scleroderma.
Circulation: P
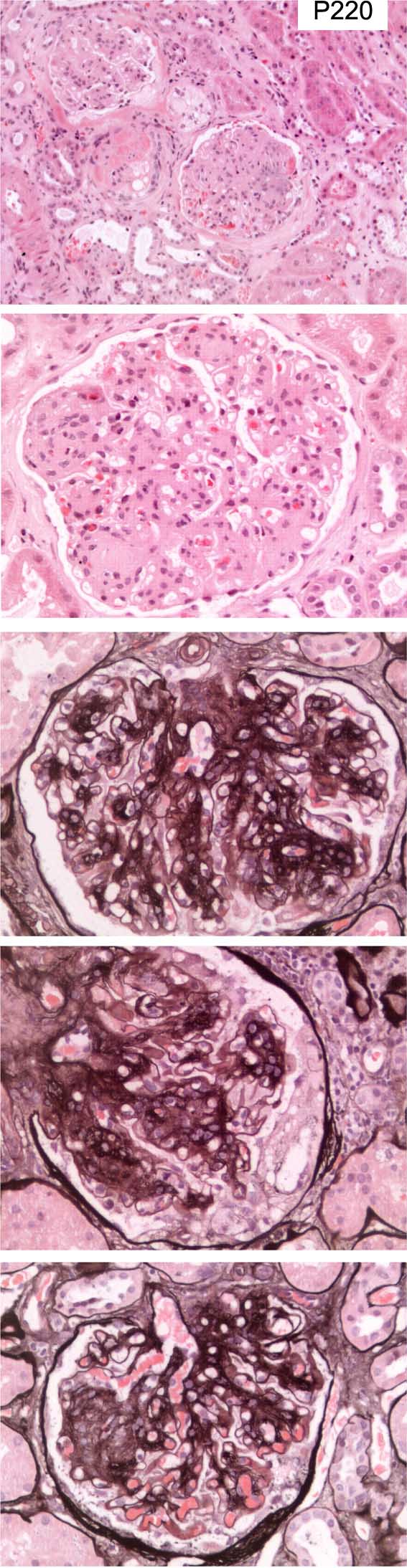
Case number: 220
....
Number of responses:79 . Date of analysis: 14 AUG 04
Clinical:
Male, 42 yrs old. Diabetic for many years with retinopathy. 8g
proteinuria. Normal renal function. Duplex kidney. IF: Small amount of
granular staining for C3 in the mesangium near the hilum. C3, IgM and C1q
present in arterioles. Otherwise negative. EM: Results not available.
Specimen:
H&E, Silver
Diagnostic categories: Score:
1 Diabetic nephropathy (nothing else mentioned) 9.67
2 Diabetic nephropathy AND ?Gn 0.20
3 Mesangiocapillary Gn type I AND diabetes 0.13
4 Amyloid? 0.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.67
Secondary diagnoses and comments (if any):
EM (reprocess if necessary)*5. Congo red*11. PAS*2. Renal immuno.*1. Immuno
for light chains*3. Should see linear IgG in diabetes.*1. Foam cells - ?
hyperlipidaemia?*1.
Original report and further information (if any):
Circulation: P
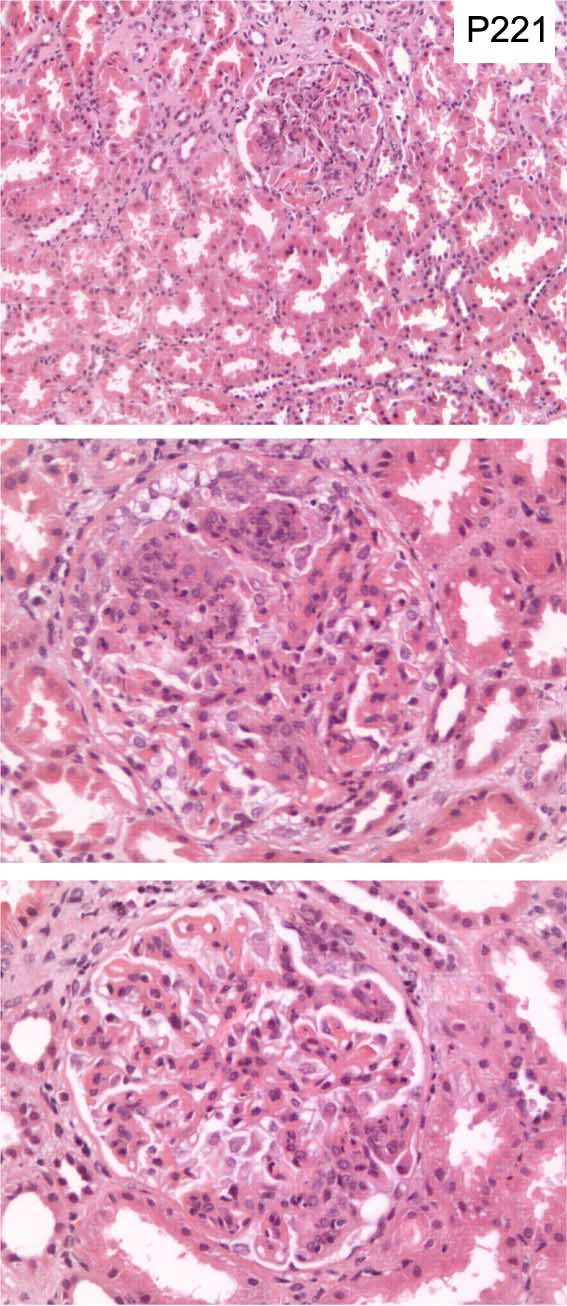
Case number: 221
....
Number of responses:79 . Date of analysis: 14 AUG 04
Clinical:
Female, 24 yrs old. Previously well, nephrotic syndrome, proteinuria 5.6g
per 24hrs, low C3 and C4. Immunofluorescence shows granular capillary
deposition of IgA, IgM, IgG, C3 and C1, affecting all parts of all six
glomeruli in the sample. The IgA staining is slightly stronger than the
other immunoglobulins and C3 is slightly stronger than C1.
Specimen:
H & E
Diagnostic categories: Score:
1 Lupus nephritis NOS 0.92
2 Lupus III and V 0.25
3 Lupus III 0.50
4 Lupus IV 6.02
5 IgA nephropathy/HSP 0.62
6 Focal segmental glomerulonephritis 0.25
7 Lupus IV and V 0.35
8 Glomerulonephritis (lupus not mentioned) 0.30
9 Dense deposit disease 0.14
10 Immune complex Gn ?lupus 0.63
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 4 with 6.02
Secondary diagnoses and comments (if any):
Lupus serology*27. Silver*9. PAS*3. EM*16. ANCA*1. Autoimmune screen*1.
Clinical evidence of lupus?*1.
Original report and further information (if any):
Reported as lupus with necrotising lesions, WHO IVB. After report issue,
anti-DNA reported positive at 1 in 80. ANCA negative, ASOT not raised.
Treated as SLE; improved. Anti-DNA subsequently fell but anti-ds-DNA
found to be positive. Creatinine never above 80.
Circulation: P
Case number: 222
....
Number of responses:79 . Date of analysis: 14 AUG 04
Clinical:
ANCA positive small vessel vasculitis in 2000. Was ANCA negative now ANCA
positive and creatinine increasing to 200. ESR and CRP increasing. ?
Vasculitis relapse.
Specimen:
H&E, PAS, Images of IgA, IgG, IgM , C9 (on CD)
Diagnostic categories: Score:
1 Vasculitis (relapse) 1.29
2 Crescentic Gn, pauci-immune/vasculitic 3.01
3 Chronic Gn (as history), no active disease 5.06
4 Cryoglobulinaemia (and damage from vasculitis) 0.13
5 IgA nephropathy 0.14
6 Post-infective Gn 0.10
7 SLE 0.01
10 Could not open CD images 0.25
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 5.06
Secondary diagnoses and comments (if any):
PAS*1. Congo red*6. MSB*2. Connective tissue stains*1. EM*9. Levels*2.
Exclude diabetes*1. Exclude anti-GBM*2. BJP*1. IEP*1. Exclude cryo.*3.
HepC?*1. ANCA titres*5. Can't exclude activity with small biopsy*5. Lupus
serology*3 Age & sex? *3. H&E too pale *5. Unsuitable for EQA*5.
Original report and further information (if any):
Circulation: P
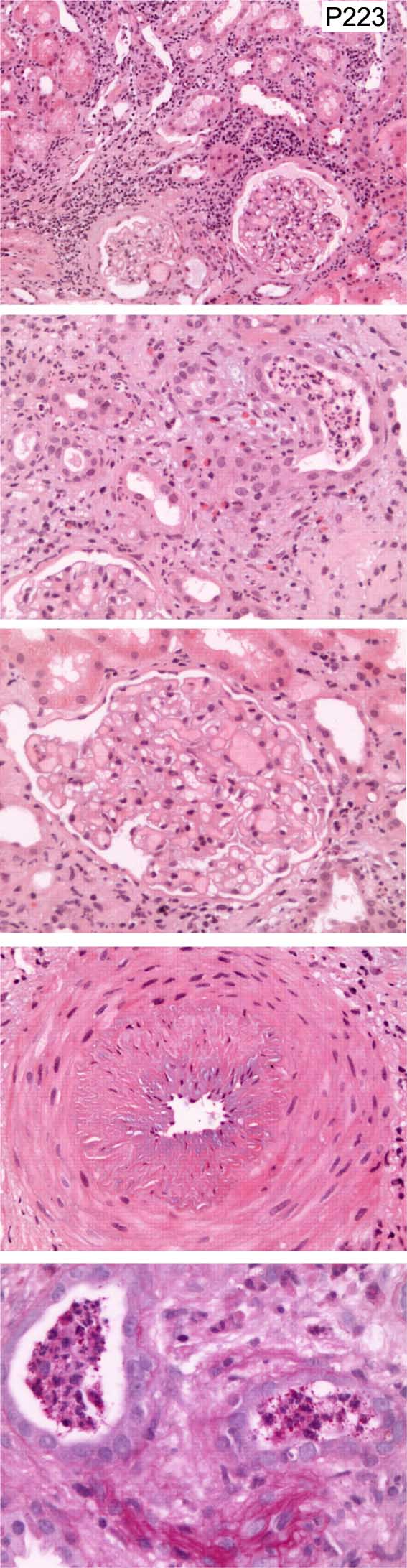
Case number: 223
....
Number of responses:78 . Date of analysis: 14 AUG 04
Clinical:
CRF, Creatinine 300, haematuria and proteinuria, immunology pending.
Immunoperoxidase showed mild mesangial IgM positivity whilst staining for
IgG, C3 and IgA was negative. EM showed mild thickening and irregularity of
the glomerular basement membranes but no electron dense deposits were seen.
No foot process effacement was seen.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Interstitial nephritis, exclude pyelonephritis 4.01
2 Interstitial nephritis NOS 2.45
3 Pyelonephritis 1.18
4 Alport syndrome 0.13
5 Renovascular disease 1.36
6 Hypertension and ascending UTI 0.50
7 Thrombotic microangiopathy 0.09
8 Mesangial proliferative Gn 0.13
9 IgM nephropathy 0.03
10 Slides not received (Organiser not informed) 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.01
Secondary diagnoses and comments (if any):
Vascular disease / hypertension too*24. ?drug related*11. Exclude
cryoglobulinaemia *2. Exclude myeloma*1. Exclude lymphoma*1. ?diabetes*1.
Odd glomerular congestion ? artefact*2. Exclude scleroderma *1. Patient
age?*15. Patient sex?*8. Elastin stain *1. Exclude UTI*4. Amount of
proteinuria?*2. Blood pressure?*1. EM*3. Unsuitable for EQA*5.
Original report and further information (if any):
Links to cases in this document:
Top
P 218
P 219
P 220
P 221
P 222
P 223
Last updated: 14 AUG 04
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk