National Renal Pathology E.Q.A. Scheme
Circulation Z
This document gives information on individual cases in
circulation Z of this scheme. It contains no personal details
of participants.
Cases included:
Z 134
Z 135
Z 136
Z 137
Z 138
Z 139
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: Z
Case number: 134 ....
Number of responses:78 . Date of analysis: 10 JAN 00
Clinical:
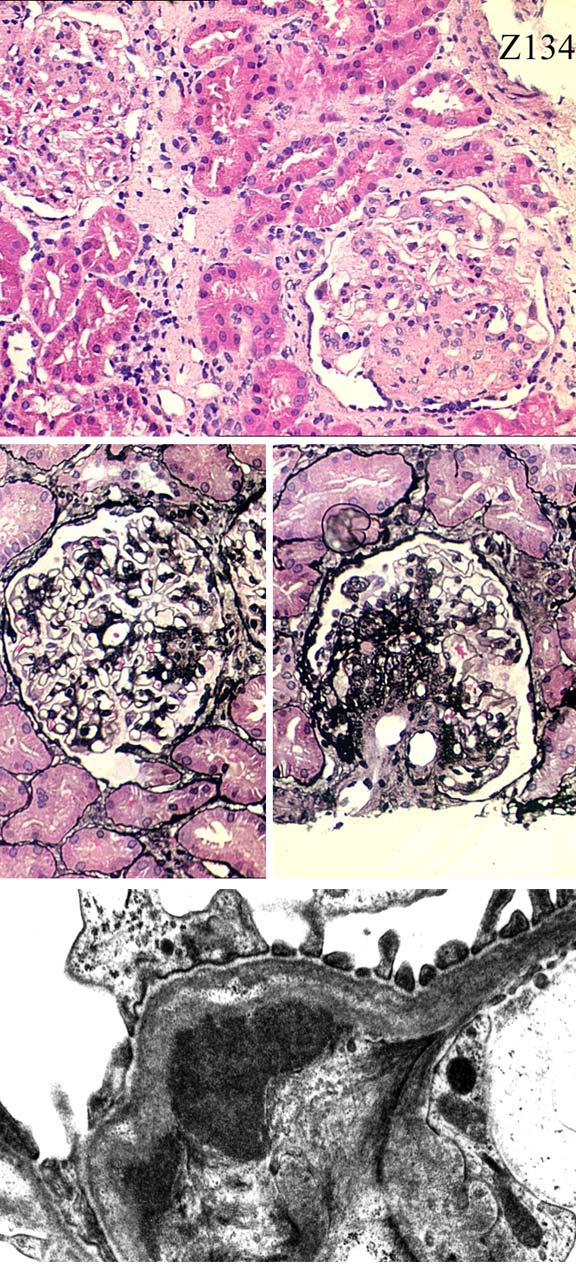
Male 37 years. Proteinuria 2.1g/24h with haematuria. Hypertensive, on
treatment. Serum autoimmune screen negative. Direct IF: Global particulate
IgA, IgM and C3 in mesangium.
Specimen:
H&E, PASilver, EMx1.
Diagnostic categories: Score:
1 IgA nephropathy 9.36
2 Mesangial proliferative glomerulonephritis 0.13
3 IgM nephropathy 0.00
4 Membranoproliferative / mesangiocapillary Gn 0.26
5 Segmental glomerulonephritis 0.13
10 No diagnosis offered 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.36
Secondary diagnoses and comments (if any):
Hypertensive vascular changes too*9. More EM*2. Formalin pigment *2.
Inadequate material for EQA/pale H&E*7. Moral: don't use plastic
coverslips!*1.
Original report and further information (if any):
IgA nephropathy.
Circulation: Z
Case number: 135 ....
Number of responses:80 . Date of analysis: 10 JAN 00
Clinical:
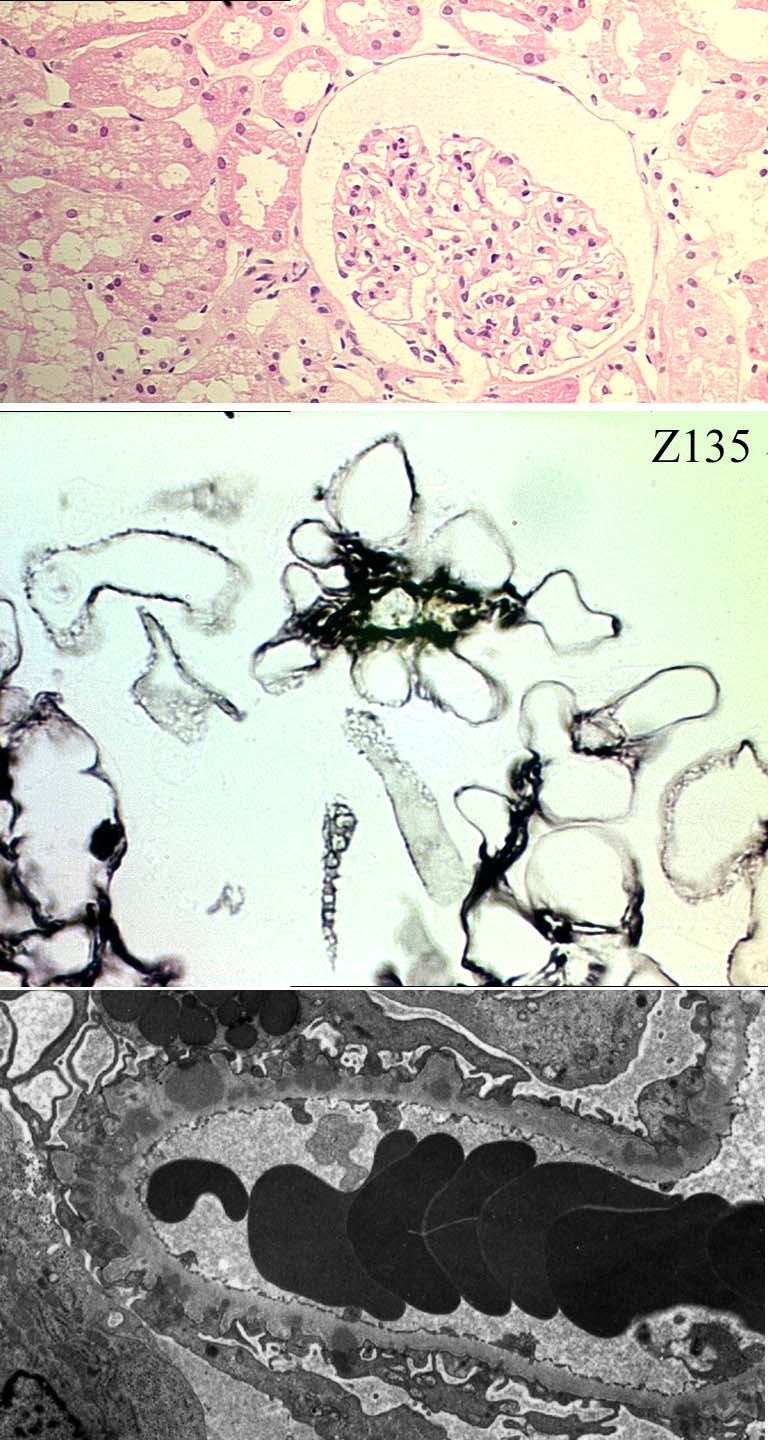
Male, 73. Routine urine examination showed proteinuria - 1g/24h. No history
of hypertension, haematuria or diabetes. Normal renal function. IgG, IgA,
C3 ++ peripheral granular deposits, IgM+/-.
Specimen:
H&E, silver, EM x1.
Diagnostic categories: Score:
1 Membranous glomerulonephritis 9.88
2 IgA nephropathy 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.88
Secondary diagnoses and comments (if any):
Poor EM*5. Exclude malignancy*7. ?Hep.B*2. ?SLE*10. Exclude drugs*4.
Original report and further information (if any):
Circulation: Z
Case number: 136 ....
Number of responses:80 . Date of analysis: 10 JAN 00
Clinical:
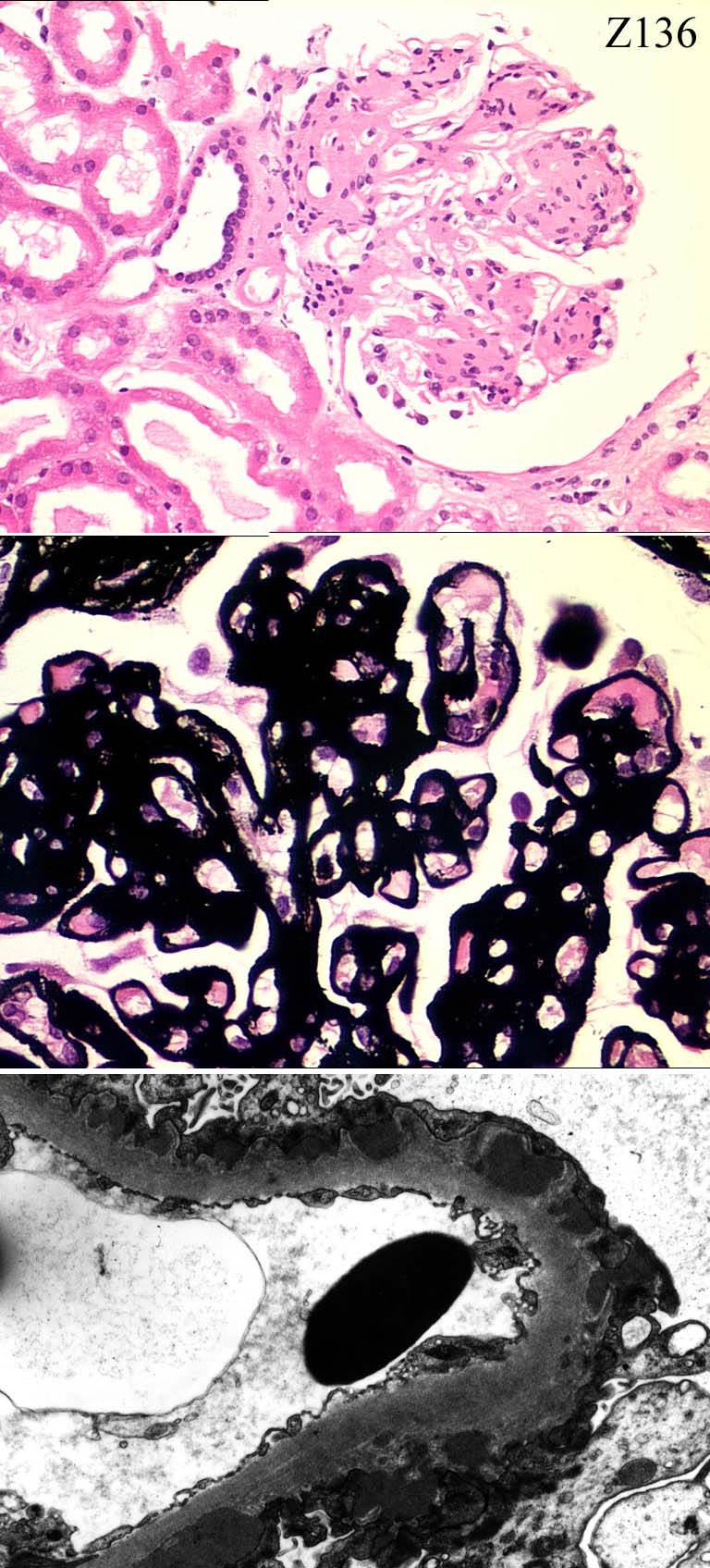
Male 56 years. Proteinuria 10g/24h, creatinine 120umol/l. Known diabetic.
Kidneys normal size. Clinical question - ?diabetic nephropathy ?other
pathology. IF: diffuse granular positivity for IgG and C3 in glomerular
capillary walls, negative for IgM, IgA and C1q.
Specimen:
H&E, PAS, MeS, EM x2.
Diagnostic categories: Score:
1 Diabetic nephropathy AND membranous Gn 9.34
2 Diabetes (membranous Gn not mentioned) 0.13
3 Membranous Gn (diabetes not mentioned) 0.21
4 Mesangiocapillary / membranoproliferative Gn 0.29
5 Diabetes and mesangiocapillary Gn 0.04
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.34
Secondary diagnoses and comments (if any):
Exclude malignancy*1. Congo red*1. Lamination of GBM on EM*1.
Original report and further information (if any):
Circulation: Z
Case number: 137 ....
Number of responses:80 . Date of analysis: 10 JAN 00
Clinical:
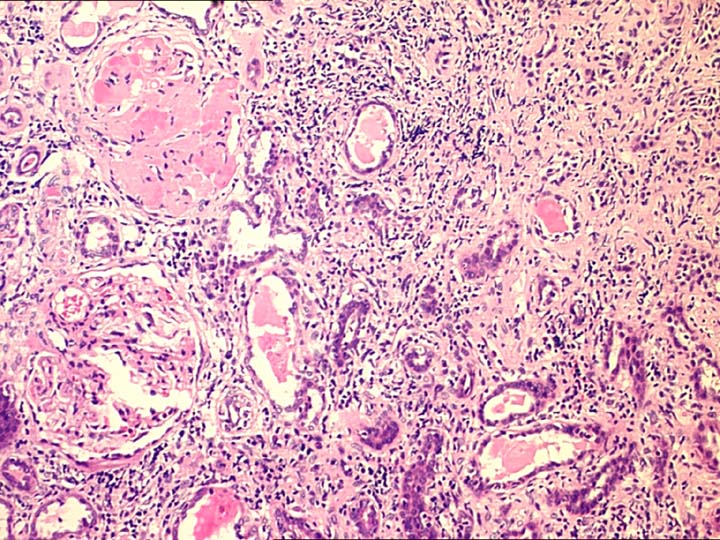
female 26. Renal failure ?cause. Uveitis. Mild asthma. Open wedge biopsy of
normal size kidney as other kidney shrunken and scarred. IF showed
mesangial IgM, +. There was C3 in segmental glomerular scars. Congo red
negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Interstitial nephritis 6.04
2 FSGS and interstitial nephritis 2.31
3 Glomerulonephritis NOS 0.01
4 Chronic pyelonephritis / reflux/scarred kidney NOS 0.33
5 FSGS 0.68
6 Monoclonal antibody deposition 0.13
7 Mesangial proliferative Gn & interstitial nephritis 0.25
8 Necrotising glomerulonephritis 0.19
9 Cryoglobulinaemia 0.04
10 Amyloidosis 0.04
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.04
Secondary diagnoses and comments (if any):
Proteinuria?*1. Consider FSGS if heavy proteinuria*5. Diabetes too?*1.
HIV status?*1. Drug induced?*7. Sjogren's?*3. ?Sarcoid*4. ?lymphoma*1.
More clinical info.*3. Silver*2. PAS*1. FSGS 2ry to hyperfiltration*6. ?
Churg-Strauss*3. ?drugs*3. ANCA?*3. Need EM*1. Kappa & lambda*2. ?
Cryoglobulin*1. ?SLE*1.
Recognised association of TIN & uveitis*21. (?Dobrin's*2.) Suitable for E
Original report and further information (if any):
Circulation: Z
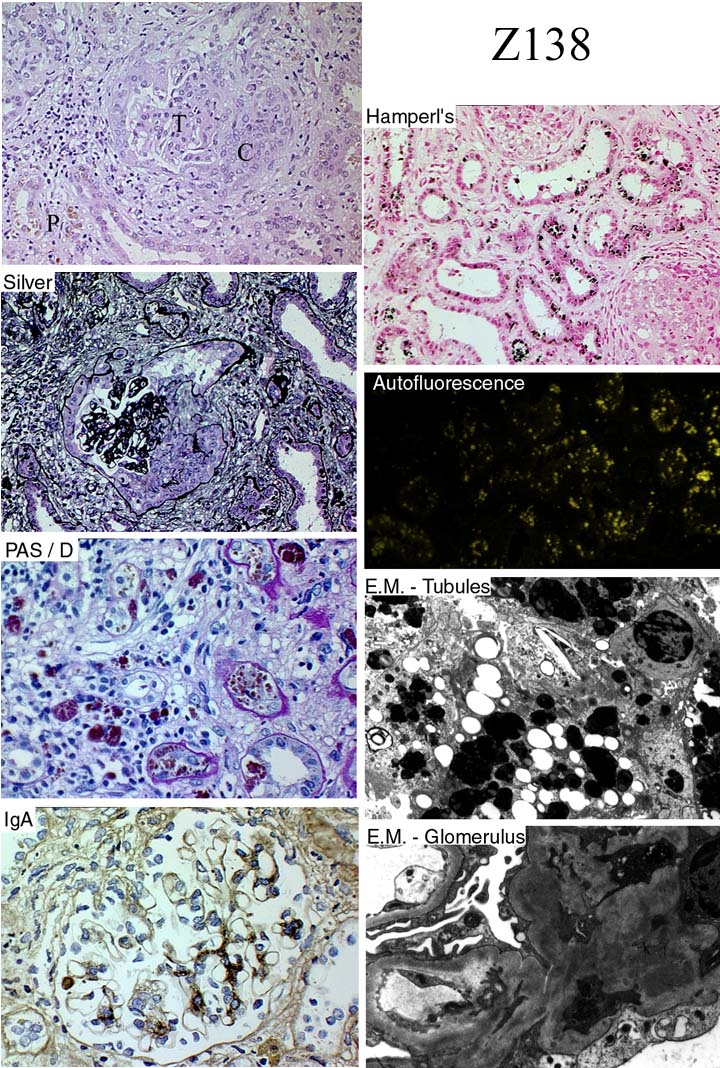
Case number: 138 ....
Number of responses:65 . Date of analysis: 10 JAN 00
Clinical:
54 y.o. woman with knowh Hermansky Pudlak syndrome (Tyrosinase-positive
albinism). Years of gradual renal impairment as expected, but sudden decline
in renal function with haematuria, therefore biopsy. FOR INTEREST NOT
PERSONAL ASSESSMENT.
Specimen:
H&E, montage of 7 labelled images
Diagnostic categories: Score:
1 Renal lesion of Herm. Pudlak AND IgA nephropathy (cresce3.38
2 Crescentic Gn & pigment / melanin in tubules 2.92
3 Crescentic IgA nephropathy / HSP 2.00
4 IgA nephropathy & interstitial nephritis 0.46
5 Crescentic Gn 0.77
6 Proliferative glomerulonephritis 0.15
7 Hermansky Pudlak syndrome 0.15
8 Crescentic Gn ? lupus & H-P syndrome ceroid 0.15
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 3.38
Secondary diagnoses and comments (if any):
No known association between Hermansky-Pudlak syndrome and IgA
nephropathy / HSP - apart from sharing the same initials??? ;-)
Original report and further information (if any):
Renal lesion of Hermansky Pudlak syndrome ('ceroid' in tubules &
macrophages, interstitial fibrosis) but also crescentic Gn due to IgA
nephropathy. Case report in progress - could the two conditions be
linked?
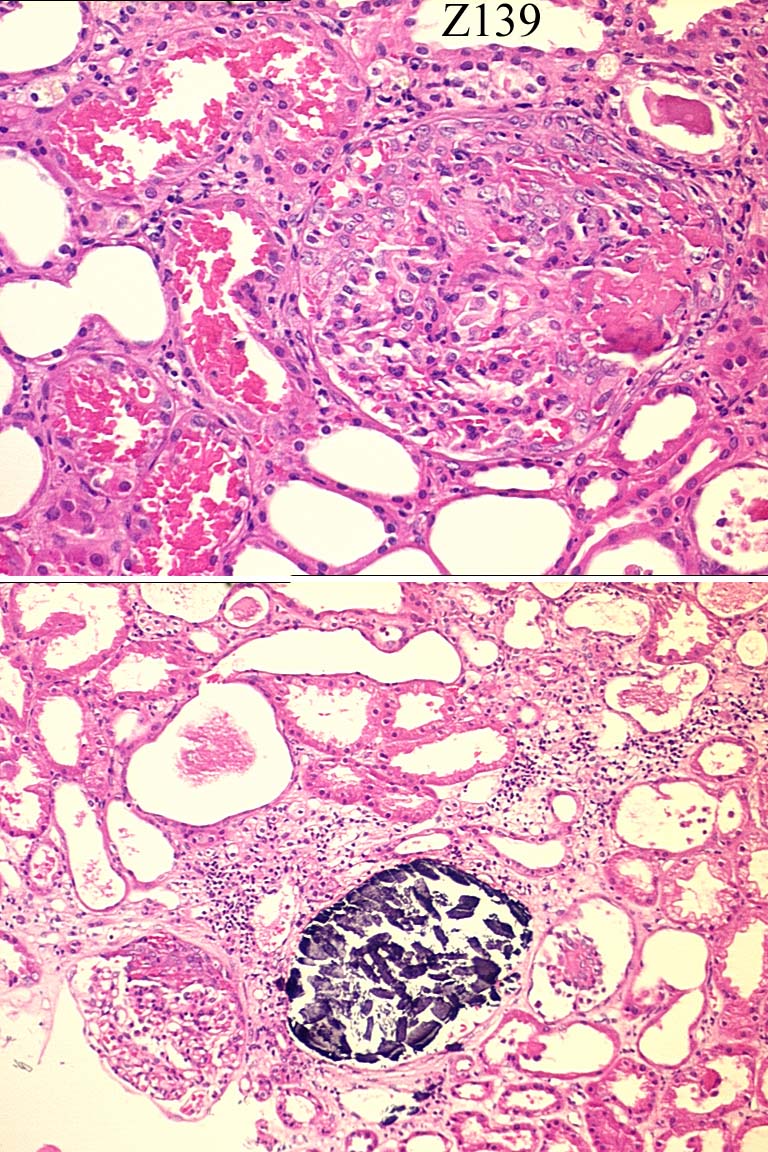
Circulation: Z
Case number: 139 ....
Number of responses:80 . Date of analysis: 10 JAN 00
Clinical:
Male age 62. Acute renal failure, dialysis dependent. MRI scan showed
'cerebral vasculitis'. E coli UTI on treatment. IF negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Pauci-immune necrotising Gn / vasculitis NOS 8.43
2 Crescentic / necrotising Gn NOS 1.13
3 TTP/HUS 0.33
4 Infective endocarditis 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.43
Secondary diagnoses and comments (if any):
ANCA*25. AntiGBM?*1. EM*1. Secondary ATN too*1. Nephrocalcinosis noted
*2. Exclude HUS*2. Exclude infection*1. Need silver*3. Need PAS*1. More
clinical info*1. Exclude SBE*1. Exclude lupus*1. Malignant hypertension?*
1. Exclude myeloma*1. Insufficient for EQA*1.
Original report and further information (if any):
Original diagnosis: Severe focal segmental nephritis consistent with
pauci-immune nephritis at pre-crescentic phase.
Links to cases in this document:
Top
Z 134
Z 135
Z 136
Z 137
Z 138
Z 139
Last updated: 10 JAN 00
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk