National Renal Pathology E.Q.A. Scheme
Circulation Y
This document gives information on individual cases in
circulation Y of this scheme. It contains no personal details
of participants.
Cases included:
Y 127
Y 128
Y 129
Y 130
Y 131
Y 132
Y 133
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: Y
Case number: 127 ....
Number of responses:61 . Date of analysis: 11 APR 99
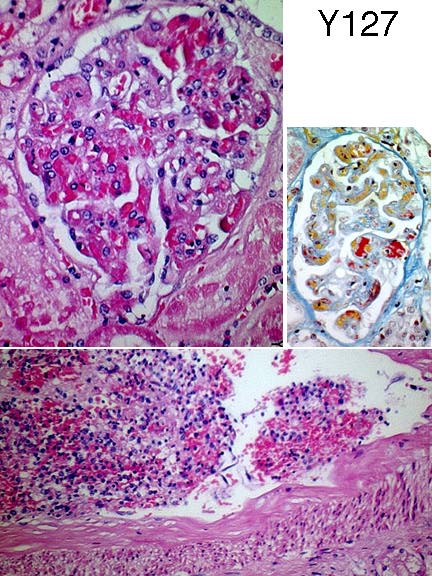
Clinical:
58year old woman, died four days after admission with infective colitis due
to E. coli 0157. Developed acute renal failure, thrombocytopenia, red cel
haemolysis and seizures. At PM kidneys (both 140g) showed multiple petechial
haemorrhages on subcapsular and cut surfaces.
Specimen:
H&E, MSB
Diagnostic categories: Score:
1 Microangiopathy (HUS/TTP etc.) 9.84
2 Renal cortical necrosis 0.16
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.84
Secondary diagnoses and comments (if any):
ATN too*5. PAS*1. Fibrinogen*1. Silver*3. EM?*1. Necrosis noted*3.
Calcification*1.
Original report and further information (if any):
Haemolytic uraemic syndrome with acute tubular necrosis and a focus of
cortical necrosis. HUS was due to infective colitis; stool culture
isolated E. coli O 157, phage type 28, toxin VT2 positive.
Circulation: Y
Case number: 128 ....
Number of responses:61 . Date of analysis: 11 APR 99
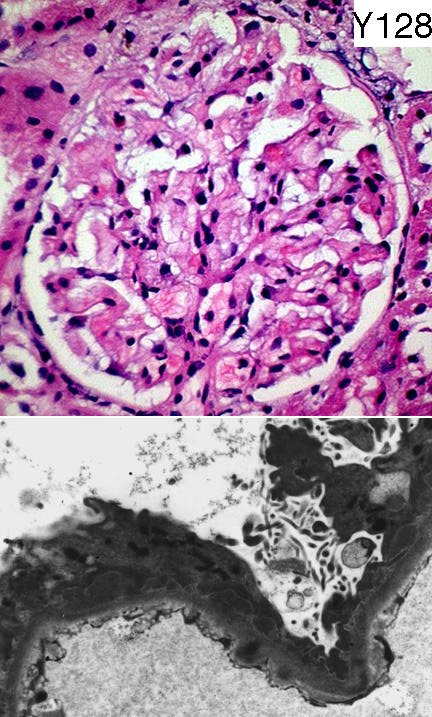
Clinical:
51 year old female. Nephrotic proteinuria with microhaematuria. Normal renal
function. Normotensive. PAS and silver showed no basement membrane
abnormality. IgG and C3- strong granular positivity along the basement
membrane. IgM less strong, same distribution.
Specimen:
H&E, EMx2.
Diagnostic categories: Score:
1 Membranous glomerulonephritis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Exclude lupus*5. Subendothelial deposits?*2. Exclude secondary membranous*
5. Poor H&E*3. A good silver should show some abnormality here*6.
Original report and further information (if any):
Membranous glomerulonephritis, stage 1.
Circulation: Y
Case number: 129 ....
Number of responses:52 . Date of analysis: 11 APR 99
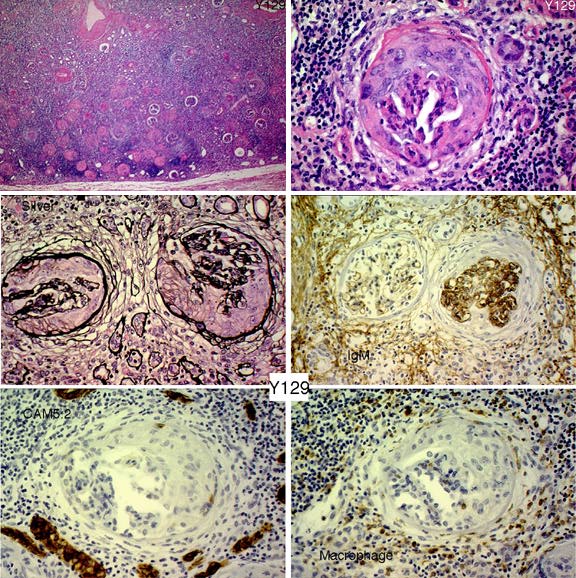
Clinical:
Female, dob. 1943. L salpingo-oophorectomy 1994. Subsequently obstructed
right kidney. Reconstructive surgery unsuccessful, right nephrectomy
performed in 1996 due to renal pain. IgM patchy, as illustrated; other Igs
negative. CASE FOR INTEREST, NOT SCORING
Specimen:
H&E, photo of silver, CAM5.2, IgM & macrophage marker
Diagnostic categories: Score:
1 Crescents as part of chronic pyelonephritis 1.73
2 Chronic scarring & crescentic Gn 1.63
3 Crescentic glomerulonephrits 1.83
4 End stage kidney NOS 1.35
5 Chronic pyelo / obstructive uropathy 2.42
6 IgM nephropathy 0.06
7 FSGS 0.04
8 Ischaemia/hypertension 0.69
9 Cryoglobulinaemia 0.06
10 Light chain / heavy chain nephropathy 0.19
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 5 with 2.42
Secondary diagnoses and comments (if any):
Hypertension too*2. Are the 'crescents' tubularisation of Bowman's space?*
2. Congo red*1. Serum antiGBM antibody?*3. Serum ANCA*6. Single organ
Wegener's?*1.
Other suggestions with no room to enter: Syphilis*1. Scleroderma*1.
Original report and further information (if any):
Glomerular 'crescents' present but probably as an unusual reaction to
reflux. Case discussed on the Internet; no better explanations. See Acta
Pathologica Japonica 34:715-26, 1984. Subsequent good course; other kidney
functioning normally, no haematuria.
Circulation: Y
Case number: 130 ....
Number of responses:61 . Date of analysis: 11 APR 99
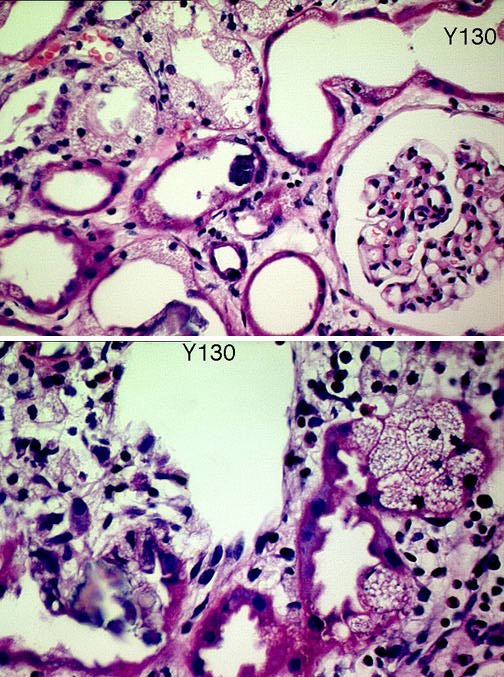
Clinical:
31y.o. male, known alcoholic, admitted extremely ill 9 days before biopsy
with haematemesis, hypotension, shock, severe acidosis, severe leukocytosis
and acute renal failure. Suggested clinical diagnoses: Vasculitis? Sepsis?
ATN?
Specimen:
H&E
Diagnostic categories: Score:
1 ATN NOS 3.93
2 ATN - toxic? 2.39
3 ATN - ischemic? 0.00
4 Vascular nephropathy 0.25
5 ATN DUE TO oxalate crystal deposition/ethylene glycol 2.30
6 ATN, oxalate crystals noted 0.82
7 Tubulo-interstitial nephritis 0.16
8 Hypovolaemia 0.16
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 3.93
Secondary diagnoses and comments (if any):
Impressive tubular vacuolation*3. Hypokalaemia?*2. Myoglobinuria?*2.
Hyperosmolar infusion?*1. Crystalline deposits ? nature*4. Urate
crystals*1. Nephrocalcinosis*1. ?potassium depletion*1. ?TIN too*1.
Original report and further information (if any):
Intratubular oxylate crystals; ethylene glycol poisoning suggested. After
recovery admitted drinking a mixture of antifreeze, surgical spirits and
methylated spirits. renal function recovered but now lost to follow-up.
Circulation: Y
Case number: 131 ....
Number of responses:61 . Date of analysis: 11 APR 99
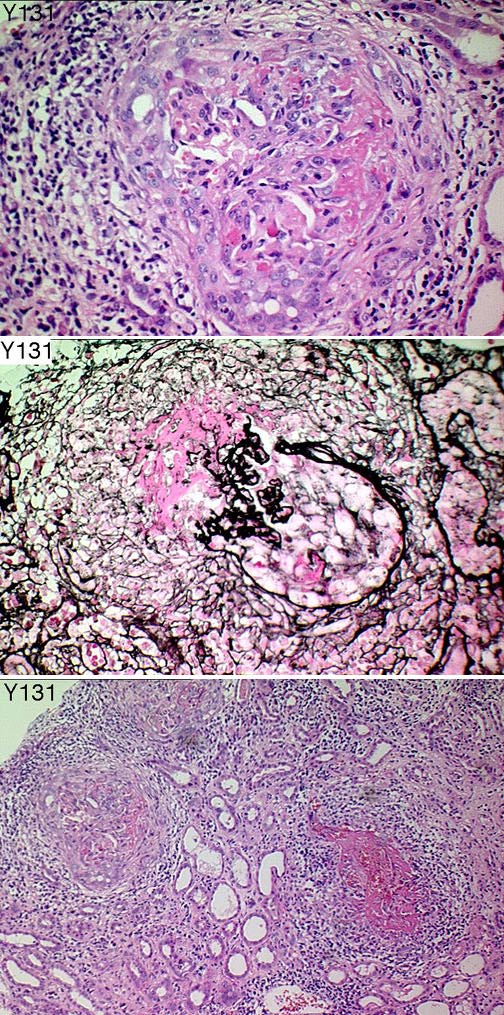
Clinical:
67 y.o. female with sudden unexplained acute renal failure. IF: linear
deposition of IgG (2+) and linear/granular deposition of C3 and C1q(2+).
Specimen:
H&E, Silver
Diagnostic categories: Score:
1 Goodpasture's disease (Anti-GBM) 9.44
2 Vasculitis / Wegener's etc. 0.07
3 Crescentic Gn NOS 0.49
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.44
Secondary diagnoses and comments (if any):
Crystals - ?urate*1. AntiGMB serology*15. ANCA*8. ANA*2. Pale H&E*3. EVG*
1. Need to see linear IF*3. Granuloma near cortical surface -
vasculitis?*1.
Original report and further information (if any):
Diagnosis: ANti-GBM disease / Goodpastures syndrome. Treated with
dialysis, plasma exchange and immunosuppression. Serum anti-GMB dropped to
normal but she never regained renal function and died with end stage renal
disease 3 months later. Never had pulmonary haemorrhage.
Circulation: Y
Case number: 132 ....
Number of responses:61 . Date of analysis: 11 APR 99
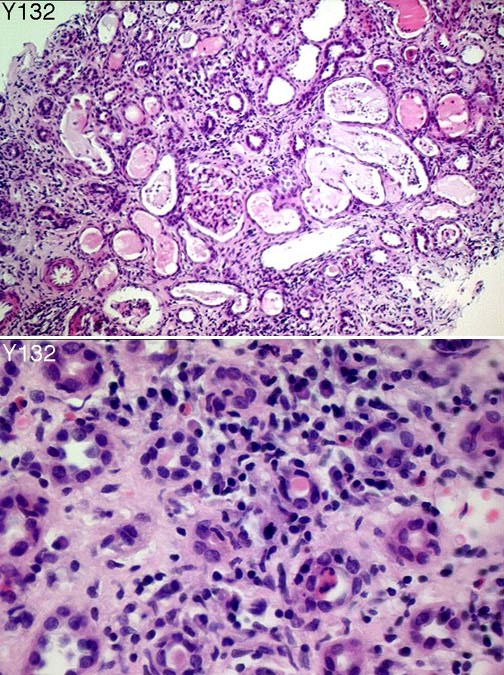
Clinical:
Female, 26. Sore throat & cervical lymphadenopathy 6 weeks ago. Now acute
renal failure, creat. 360. Otherwise very well! Clinical - ?acute Gn,
vasculitic or lupus? Immuno. negative, basmement membrane normal on silver
stain. Only drugs were hyoscine & mebeverine for irritable bowel. Raised se
Specimen:
H&E
Diagnostic categories: Score:
1 Interstitial nephritis 9.61
2 Acute pyelonephritis 0.20
3 Myeloma cast nephropathy 0.16
4 Myoglobinuria 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.61
Secondary diagnoses and comments (if any):
Drug induced?*17. Sarcoid / ACE levels?*1. Related to viral infection?*4.
Exclude acute pyelo*3. Exclude paraprotein*2. Exclude lupus*1. EVG*1.
Original report and further information (if any):
Initial diagnosis: tubulo-interstitial nephritis, probably drug induced;
exclude renal infection. Treated with steroids,recovered normal renal
function. MSU and blood cultures negative. Admitted ibuprofen use when
questioned.
Subsequent uveitis - could it be Dobrin's syndrome??? Sarcoidosis??? - u
Circulation: Y
Case number: 133 ....
Number of responses:44 . Date of analysis: 11 APR 99
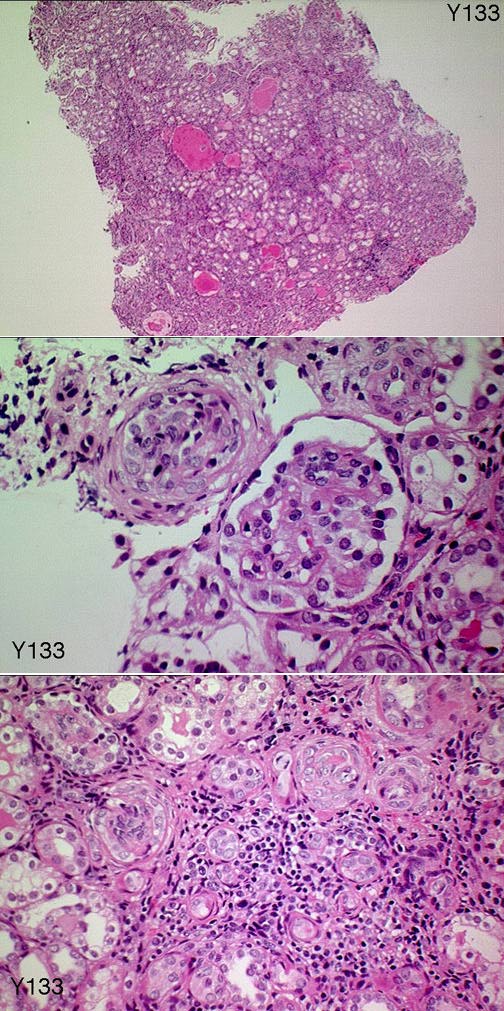
Clinical:
3 month old girl. Congenital nephrotic syndrome. Open renal biopsy. No
further information provided. (NOTE: Case from outside U.K. This may or may
not be relevant to the diagnosis - PF). Case submitted for interest, not
EQA.
Specimen:
H&E CASE FOR INTEREST, NOT EQA
Diagnostic categories: Score:
1 Congenital nephrotic syndrome - Finnish type 5.16
2 Congenital nephrotic syndrome - French type 0.45
3 Congenital nephrotic syndrome, diffuse mesangial scleros2.91
4 Nail-patella syndrome 0.11
5 Denys-Drash syndrome 0.45
6 Congenital syphilis 0.45
7 Proliferative glomerulonephritis 0.23
8 Dysgenetic kidneys 0.23
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.16
Secondary diagnoses and comments (if any):
Need more clinical info*2. E.M.*1. PAS*1. Family history?*1. HIV?*1. Was
placenta normal?*1.
Original report and further information (if any):
Presented 2/12 old with puffy face and bilateral renal masses. Initial
clinical diagnosis ARPKD. Serum albumin 7g/l, 24h u.protein 520mg, creat
166umol/l. Biopsy diagnosis: Congenital nephrotic syndrome, Finnish type.
Parents declined further treatment, no follow up available.
Links to cases in this document:
Top
Y 127
Y 128
Y 129
Y 130
Y 131
Y 132
Y 133
Last updated: 11 APR 99
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk