National Renal Pathology E.Q.A. Scheme
Circulation X
This document gives information on individual cases in
circulation X of this scheme. It contains no personal details
of participants.
Cases included:
X 121
X 122
X 123
X 124
X 125
X 126
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: X
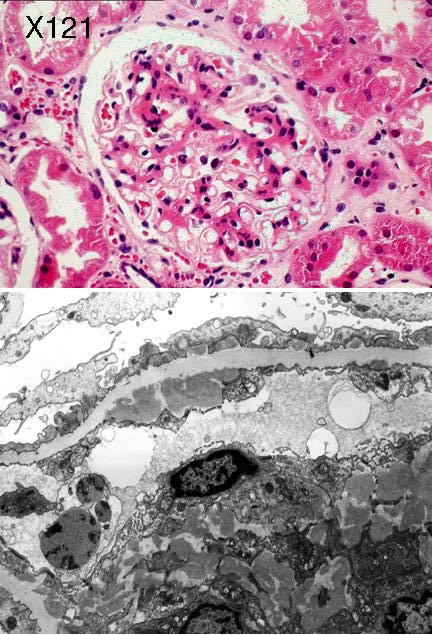
Case number: 121 ....
Number of responses:61 . Date of analysis: 11 APR 99
Clinical:
Male 17 years, acute nephrotic syndrome, albumin 16, ++++protein, +blood,
creatinine 84, pancytopenia & splenomegaly. IF.: IgA++, IgG++, IgM++,
C1q++, C3++, C4++, all with granular deposition, mesangium and periphery.
Specimen:
H&E, E.M.x1
Diagnostic categories: Score:
1 Lupus nephritis NOS 0.49
2 Lupus nephritis focal prolif (WHO2) 1.46
3 Lupus nephritis diffuse prolif (WHO3) 3.21
4 Lupus nephritis (WHO 4) 2.26
5 Lupus nephritis (WHO 5) 0.69
6 Post-infectious Gn 0.02
7 IgA nephropathy / Henoch Schonlein 0.70
8 Gn NOS, probably lupus 0.66
9 Mesangiocapillary Gn 0.51
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 3.21
Secondary diagnoses and comments (if any):
Lupus serology*18. Silver stain*3. Trichrome*1. Clinical info.*2.
Inadequate biopsy *7.
Original report and further information (if any):
Provisional: Mesangiocapillary glomerulonephritis, probably due to lupus.
Final conclusion: Lupus nephritis, WHO III. Started Pred. & Aza. 18
months later still heavy proteinuria (7g/24h) but not clinically
nephrotic; creatinine 76.
Circulation: X
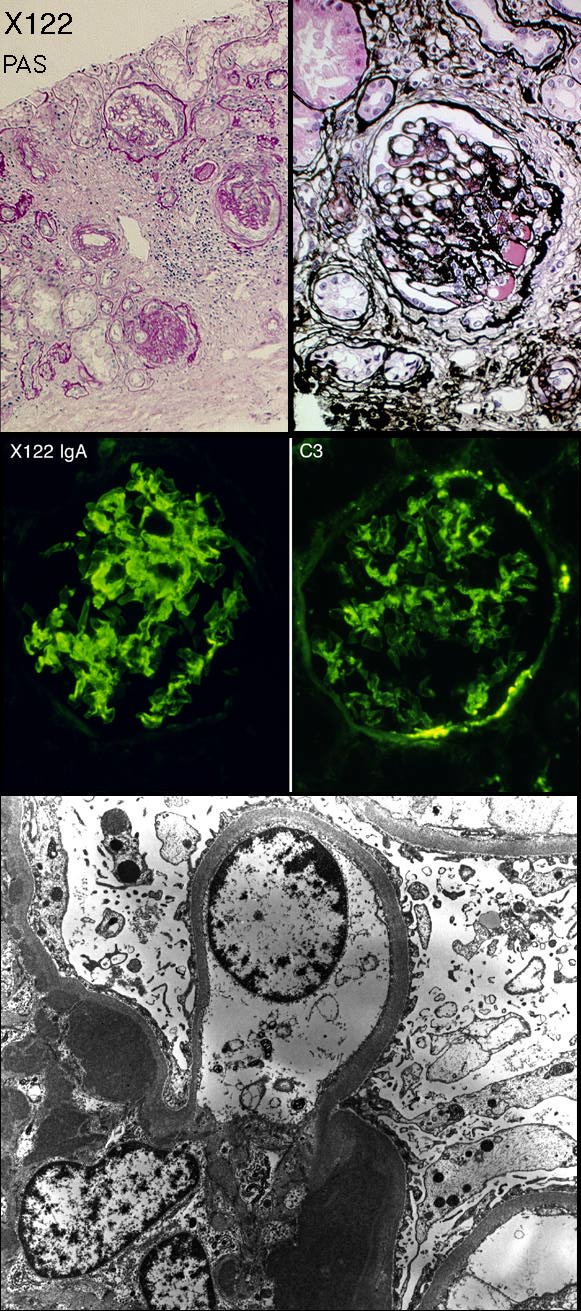
Case number: 122 ....
Number of responses:62 . Date of analysis: 11 APR 99
Clinical:
Male, 31. Incidental finding, proteinuria (8.8g/l) and HT 1 year.
Clinically asymptomatic. Previosuly thrombocytopenic. Also NIDDM &
schizophrenia. On Metformin & Enalapril. ANF and ANCA negative. Creatinine
90. (Case from Hong Kong. This may be irrelevant - PF)
Specimen:
PASM(H&E); PAS; Transp. IgA & C3; EMx2
Diagnostic categories: Score:
1 IgA nephropathy 9.69
2 Henoch Schonlein purpura 0.23
3 FSGS 0.08
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.69
Secondary diagnoses and comments (if any):
Is other immuno. negative?*3. Nephrotic presentation unusual*3. Consider
diabetes too (thick GMB)*7. Hypertension too*3. Ischaemia too*1. H&E*3.
ASOT*1.
Original report and further information (if any):
IgA nephropathy, CUHK-PWH Grade 2, tubulo-interstitial grade 2.
Hypertensive hyalinization and early diabetic glomerulosclerosis also
present. Reference: Modern Pathology 6:684-690, 1993.
Circulation: X
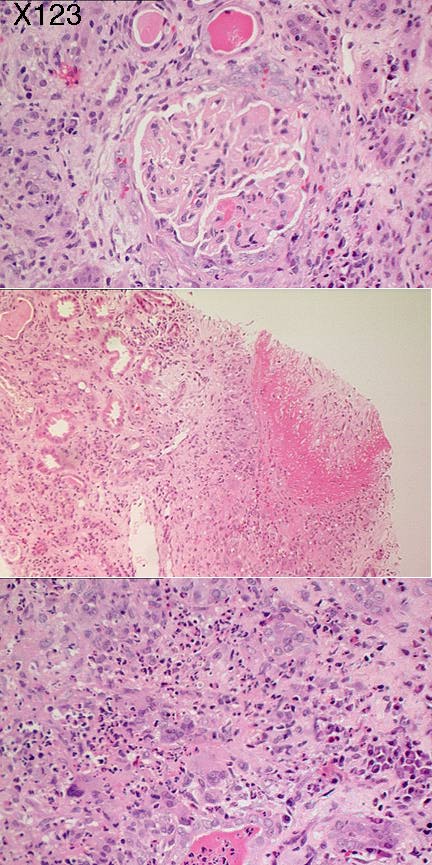
Case number: 123 ....
Number of responses:62 . Date of analysis: 11 APR 99
Clinical:
65y.o. man presented with atypical pneumonia, found to have proteinuria and
haematuria with rapidly deteriorating renal function. On transfer to renal
physicians, creatinine 400, C-ANCA positive, skin rash. IF and peroxidase
showed IgM, C3 and fibrinogen in glomeruli and blood vessels. IgG and IgA
Specimen:
H&E x2 (labelled A1 & A2)
Diagnostic categories: Score:
1 Vasculitis NOS 2.51
2 Polyarteritis 0.68
3 Wegener's 6.65
4 Post-infectious glomerulonephritis 0.16
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 6.65
Secondary diagnoses and comments (if any):
Exclude cryoglobulins*1. Exclude infection/UTI*3. PAS*1. Silver*3. EVG*2.
Trichrome*1. Anti-GBM antibody*1. ATN too*3. Granulomatous interstitial
nephritis*3. H&E too pale*3.
Original report and further information (if any):
Biopsy diagnosis Wegener's granulomatosis. Subsequently developed
vasculitic rash, respiratory symptoms & nasal bleeding. Good recovery on
steroids & cyclophosphamide - creatinine now 200. ANCA now negative.
Circulation: X
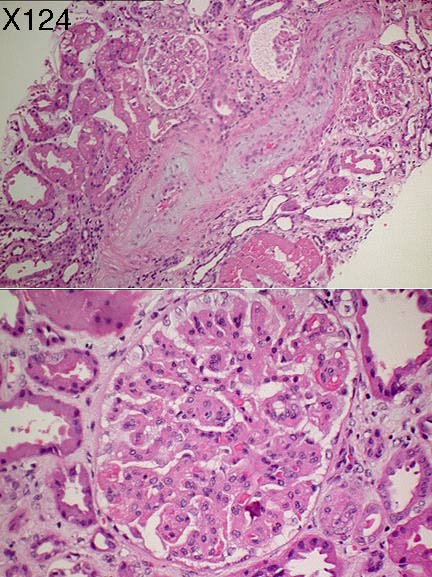
Case number: 124 ....
Number of responses:62 . Date of analysis: 11 APR 99
Clinical:
Female aged 37. Diagnosed hypertensive in 1997. Presented 7/5/98 with
rapidly deteriorating renal function despite treatment. IF negative for
IgA, G, M and C3.
Specimen:
H&E
Diagnostic categories: Score:
1 Malignant hypertension / scleroderma 5.08
2 Hypertension (+/- malignant) 1.66
3 Scleroderma 1.02
4 Microagniopathy (HUS, TTP etc.) 1.49
5 Hypertension / microangiopathy 0.76
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.08
Secondary diagnoses and comments (if any):
HT / scleroderma / microangiopathy differential requires clinical
information*15. ATN too*4. Platelet count*1. Neurological symptoms?*1.
Clinical scleroderma?*6. Pregnancy?*2. EM*4.Serology*1. Antiphospholipid
antibody*1. ANCA*1. Inadequate material*2. PAS*2. Silver*2. Trichrome*1.
IF for fibrin?*1. Exclude lupus*1.
Original report and further information (if any):
Patient died 1 month after biopsy following haematemesis. P.M.: 450g
heart, pulmonary oedema, 2cm bleeding gastric ulcer, focal acute
pancreatitis & fatty liver. No evidence of systemic sclerosis. Death
attributed to malignant hypertension & gastro-intestinal haemorrhage.
Circulation: X
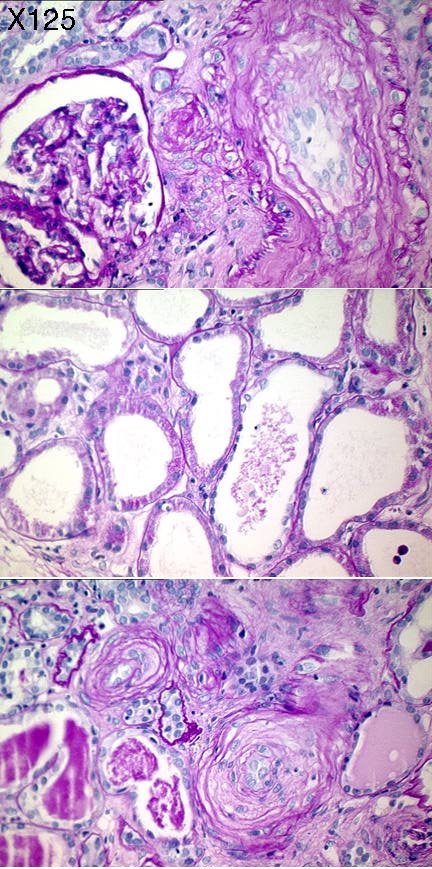
Case number: 125 ....
Number of responses:62 . Date of analysis: 11 APR 99
Clinical:
Male aged 57, employed London Transport. Gave up smoking 10y ago.
Hypertention 12 months previously but not treated. Presents in ARF, creat.
1074, severe hypertension. ANCA -ve. No clinical scleroderma. IF: C3 in
vessels. IgA flecksin vessels & tubules. IgG&M negative. Fibrin flecks, int
Specimen:
PAS diastase (Contributor deliberately omitted H&E)
Diagnostic categories: Score:
1 Hypertension 8.63
2 Microangiopathy / HUS etc. 0.85
3 Scleroderma 0.16
4 Dermatomyositis 0.03
5 Ischaemia & benign degenerative vasculopathy 0.31
6 Myeloma kidney/cast nephropathy 0.02
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.63
Secondary diagnoses and comments (if any):
ATN too*1. Exclude microangiopathy*5. 'Microangiopathy - probably due to
hypertension'*1. Exclude vasculitis*1. Interstitial nephritis too*1. Poor
section - ? adequate*2. Objection about no H&E*14. Exclude myeloma*4.
Exclude scleroderma*9. Serology*1. EM*3. MSB*2.
Original report and further information (if any):
Original report: Changes due to accelerated hypertension.
Patient had been noted to be hypertensive 1 year earlier but no action was
taken. Anuric & on dialysis at time of biopsy. IF and EM subsequently
showed no evidence of a primary glomerular disorder.
Circulation: X
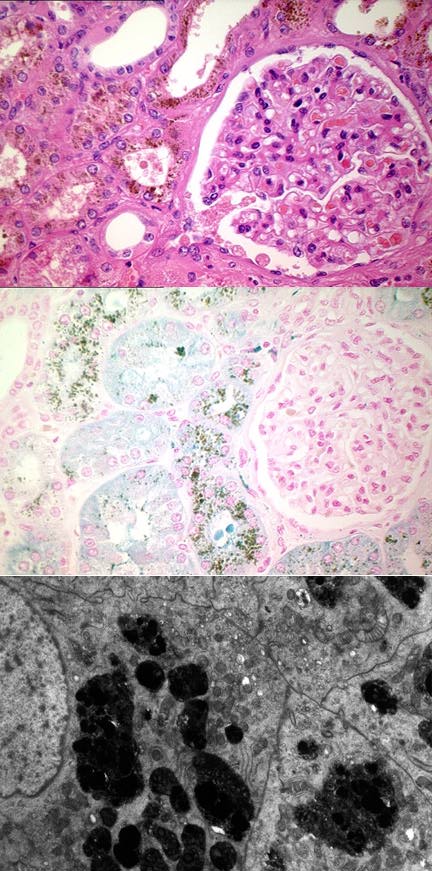
Case number: 126 ....
Number of responses:54 . Date of analysis: 11 APR 99
Clinical:
Female, 67. Prosthetic heart valve (reason not stated) and murmur- probably
due to leak round valve. Proteinuria 3g/24h and mild impairment of renal
function - due to mild heart failure?? Bled after biopsy (on Warfarin!!)
therefore nephrectomy. Immunoperoxidase negative. FOR INTEREST, NOT SCORIN
Specimen:
H&E, Perl's, EM - glom.x1, tubulex1.
Diagnostic categories: Score:
1 Haemosiderosis / haemolytic anaemia (traumatic) 4.91
2 Benign nephrosclerosis 0.19
3 Mesangial proliferative Gn 0.19
4 Haemosiderosis due to venous congestion 0.19
5 Haemosiderosis NOS 3.33
6 Haemosiderosis due to warfarin treatment/renal bleeding 0.46
7 Haemochromatosis 0.19
8 Aminoglycoside toxicity 0.19
9 Nephropathy of cyanotic heart disease 0.19
10 Tubular deposition of plastic from prosthesis 0.19
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.91
Secondary diagnoses and comments (if any):
Minimal change nephrotic syndrome too*5. More e.m.*2. Stain for
lipofuscin*1. Masson*2. Exclude storage disorder*1. Exclude
haemochromatosis *1. Exclude blackwater fever(???!!)*1. More clinical
info.*1.
Other diagnoses (no room): Renal melanosis *1. Granular tubular hyalinosis
Original report and further information (if any):
Massive tubular haemosiderosis due to erythrocyte rupture by defective
heart valve & haemoglobinaemia. Casue of proteinuria unclear - minimal
change?? No haemosiderin in podocytes. Proteinuria resolved after
replacement of prosthetic heart valve.
Links to cases in this document:
Top
X 121
X 122
X 123
X 124
X 125
X 126
Last updated: 11 APR 99
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk