National Renal Pathology E.Q.A. Scheme
Circulation V
This document gives information on individual cases in
circulation V of this scheme. It contains no personal details
of participants.
Cases included:
V 109
V 110
V 111
V 112
V 113
V 114
End
A click on the  icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: V
Case number: 109 ....
Number of responses:70 . Date of analysis: 28 JUL 98
Clinical:
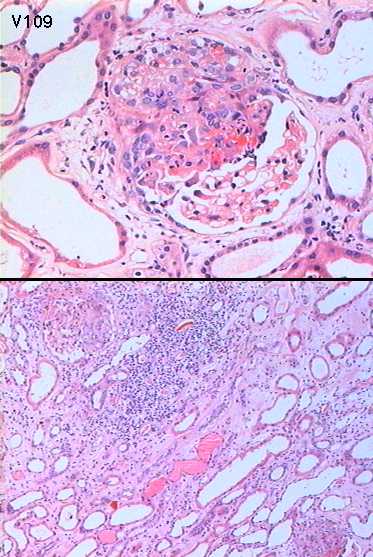
74y.o. male. Long history ischaemic heart disease and asthma. Admitted 'on
take' with short history of peripheral neuropathy. Acute renal failure - Ur
32, creatinine 415. p-ANCA +ve (1:80) MPO-ANCA weak +ve. c-ANCA and anti-GBM
negative. IF and IP negative. EM necrosis and ischaemic changes.
Specimen:
H&E
Diagnostic categories: Score:
1 Pauci-immune necrotising Gn / vasculitis 9.29
2 Extracapillary proliferative Gn with crescents 0.14
3 Churg Strauss syndrome 0.43
4 Focal segmental proliferative glomerulonephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.29
Secondary diagnoses and comments (if any):
ATN too*8. Arteriosclerosis too*8. Interstitial nephritis too*3. Hep B
surface Ag.?*1. Elastin stain*2. A few eosinophils, not enough for Churg
Strauss*1.
Original report and further information (if any):
Pauci-immune focal segmental necrotising glomerulonephritis. pANCA
positive, 1:80. Imunosuppressed. Renal function improved but re-admitted
with lung consolidation - died. At P.M. - pneumocystis pneumonia and
invasive aspergillosis.
Circulation: V
Case number: 110 ....
Number of responses:70 . Date of analysis: 28 JUL 98
Clinical:
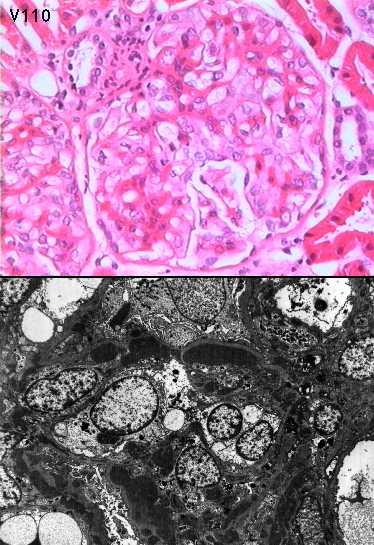
28y.o. man with history of SLE. Presented with haematuria and proteinuria.
Immunofluorescence showed strong granular positivity for IgG and C3,
predominantly in a loop distribution. IgM was positive to a lesser degree.
Specimen:
H&E, E.M.x2.
Diagnostic categories: Score:
1 Lupus nephritis NOS 1.14
2 Lupus nephritis, WHO II 0.74
3 Lupus nephritis, WHO III 1.79
4 Lupus nephritis, WHO IV / diffuse proliferative 4.29
5 Lupus nephritis, WHO V / membranous 1.61
6 Membranous Gn (lupus not mentioned) 0.43
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 4 with 4.29
Secondary diagnoses and comments (if any):
Silver stain*7. Better H&E*3. Need more material for accurate WHO
classification*3.
Original report and further information (if any):
Proliferative lupus nephritis
Circulation: V
Case number: 111 ....
Number of responses:70 . Date of analysis: 28 JUL 98
Clinical:
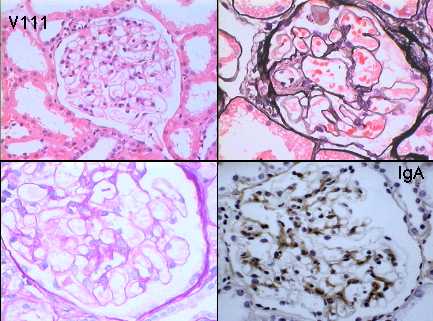
Asian male, 40 y.o. Generalised vasculitis. ANCA negative. Haematuria.
Biochemistry normal. Immunoperoxidase: IgG and IgM negative. IgA and C3
provided.
Specimen:
H&E, PAS, Silver, proj. slides of IgA and C3
Macro:
0.9cm needle core
Diagnostic categories: Score:
1 IgA nephropathy 7.06
2 Henoch Schonlein disease 2.92
3 Lupus nephritis 0.01
10 1 and 2 to merge before scoring - PNF 0.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.06
Secondary diagnoses and comments (if any):
IgA nephropathy despite normal l.m. *3. LM normal therefore IgA depsosits
are clinically irrelevant*3. Levels *1. EM*4. Bx skin rash *1. Peroxidase
difficult to interpret*1. Link between 'generalised vasculitis(??) and
glomerular IgA cannot be assumed*2. ?ATN too*1.
Original report and further information (if any):
Circulation: V
Case number: 112 ....
Number of responses:70 . Date of analysis: 28 JUL 98
Clinical:
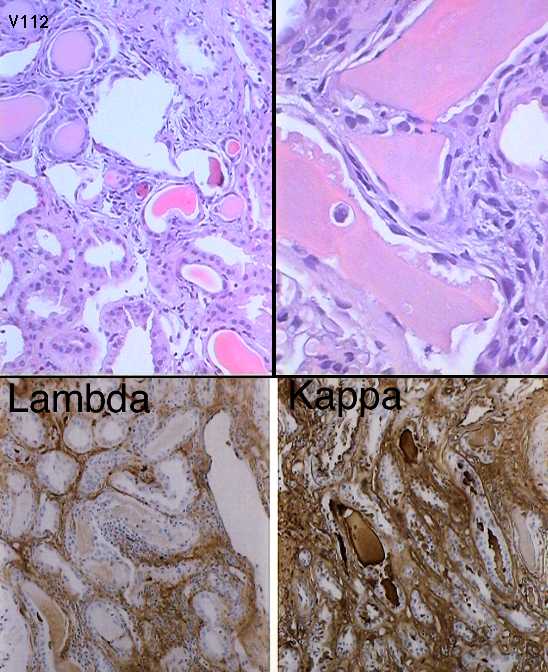
44y.o. male, acure renal failure & proteinuria. Creatinine 750, 6.8g
proteinuria/24h. X ray multiple destructive bone lesions.No M-componenet on
serum electrophoresis. Clinically ?amyloid,?myeloma kidney, ?light chain
deposition, ?toxic damage (ingested NSAIDs+++) IPx -ve for Igs & complement.
Specimen:
H&E, PAS, photo of kappa & lambda
Diagnostic categories: Score:
1 Myeloma kidney (cast nephropathy) 9.29
2 Tubulo-interstitial nephritis 0.00
3 Light chain disease 0.71
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.29
Secondary diagnoses and comments (if any):
Prolifeative Gn too*1. EM for light chain nephropathy*3. Exclude amyloid *
8. Chronic vascular disease*1. Kappa positive interstitial infiltrate too*
1. Bone marrow? Repeat serum immunoelectrophoresis? Bence Jones
proteinuria?*2.
Original report and further information (if any):
Myeloma kidney. Clinical diagnosis light chain multiple myeloma, stage 3b.
Proteinuria (2.5g/l) was exclusively due to free kappa light chain
excretion.
Circulation: V
Case number: 113 ....
Number of responses:56 . Date of analysis: 28 JUL 98
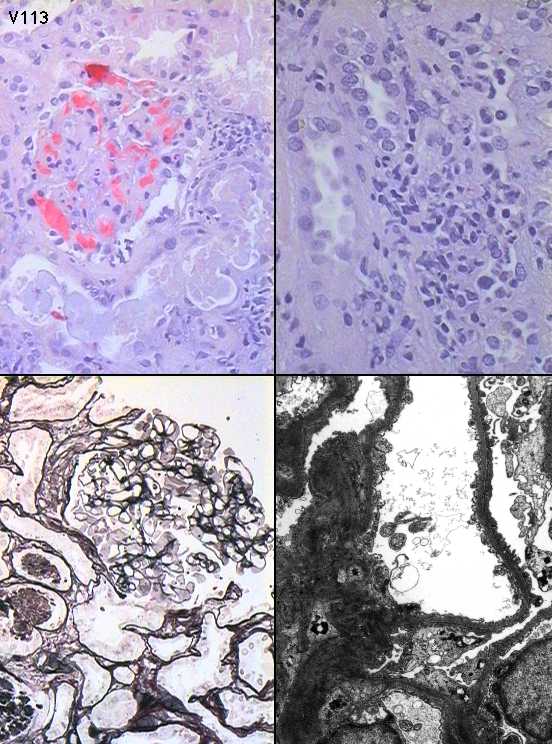
Clinical:
65y.o. male, ARF and nephrotic syndrome.Upper respiratory tract infection 3
weeks before admission. At biopsy, creatinine 457, urine protein 12.2g/24h.
Hypertensive, on treatment for years. No other clinical history. Clinical
diagnosis RPGn. Immuno: no specific staining for Igs or complement. FOR IN
Specimen:
H&E, PAS, Silver, E.M. *2. FOR DISCUSSION NOT EQA
Diagnostic categories: Score:
1 Minimal change nephropathy 3.08
2 Tubulo-interstitial nephritis 1.52
3 Interstitial nephritis/toxic damage AND minimal change 3.39
4 IgA nephropathy 0.09
5 Proliferative glomerulonephritis 0.27
6 Myeloma / light chain nephropathy 0.27
7 Chronic pyelonephritis 0.04
8 Renovascular disease 0.18
9 Mesangiocapillary glomerulonephritis 0.09
10 No response received 1.07
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 3.39
Secondary diagnoses and comments (if any):
Unsuitable / insufficient for EQA*7. Congo red*1. Kappa & lambda*2. Exclude
lymphoproliferation/malignancy*2. Hypertensive damage too*4. Pleomorphic
nuclei - ?B12/folate?*1. Drug related?*4. Exclude renal vein thrombosis*
1. ?Acue pyelonephritis too *5. ATNtoo *3.
Original report and further information (if any):
Minimal change nephrotic syndrome with acute tubular damage and slight
interstitial nephritis, suggesting a toxic renal injury, probably due to
NSAIDs or other drugs. Patient admitted Diclofenac abuse. Recovered after
biopsy without specific therapy.
Circulation: V
Case number: 114 ....
Number of responses:69 . Date of analysis: 28 JUL 98
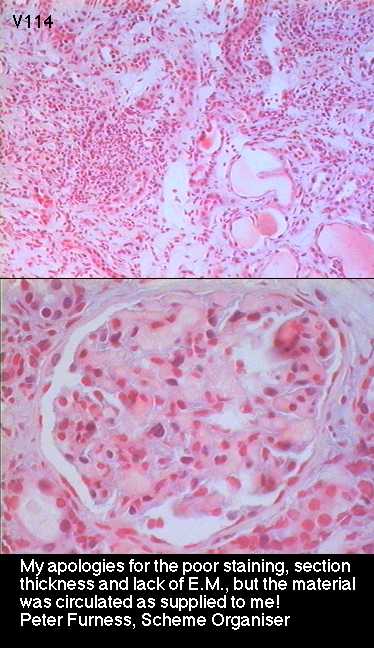
Clinical:
65 y.o. female. Initially no history! At case conference - mild to moderate
acute renal impairment, proteinuria. History of musculo-skeletal problems
including 'arthritis'. IF negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Interstitial nephritis 8.34
2 Mixed connective tissue disease 0.14
3 Myeloma kidney 0.78
4 Urate nephropathy 0.07
5 Amyloidosis 0.08
10 No diagnosis (inadequate material etc.) 0.58
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.34
Secondary diagnoses and comments (if any):
Awful section/stain*39. Unsuitable for EQA*21. Section stained in tea?*1.
Unprintable comments about quality of section*4.
Re-do IF*1. Exclude myeloma*7. Exclude amyloid*2. ?lymphoma*1. NSAIDs/
drugs related?*21. Immuno for light chains*2. ?scleroderma*1. ?Gn too??*
1.
Original report and further information (if any):
Had received NSAIDs for 'rheumatism'. Recovered after treatment with
steroids and support for renal failure.
Links to cases in this document:
Top
V 109
V 110
V 111
V 112
V 113
V 114
Last updated: 28 JUL 98
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk