National Renal Pathology E.Q.A. Scheme
Circulation U
This document gives information on individual cases in
circulation U of this scheme. It contains no personal details
of participants.
Cases included:
U 103
U 104
U 105
U 106
U 107
U 108
End
A click on the  icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: U
Case number: 103 ....
Number of responses:58 . Date of analysis: 16 DEC 97
Clinical:
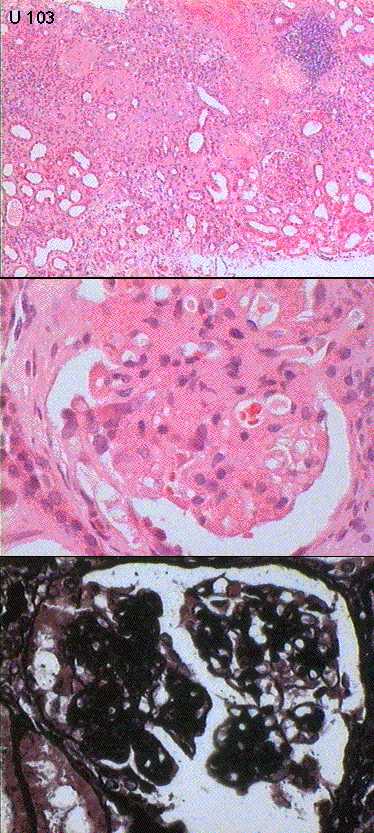
69y.o. male with lethargy, malaise,nausea & vomiting for 2 months. Treated
for hypertension. Urea 50, creat.1088, Na135, K 8.5, BP212/100. Leg
claudication 18 months. RF, ANA, DNA, ANCA all neg. IF: moderate but
variable granular IgA, lesser C3, mesangium and capillary loops. Some IgM in
Specimen:
H&E, Methenamine silver
Diagnostic categories: Score:
1 IgA nephropathy 8.38
2 Mesangial proliferative glomerulonephritis 0.17
3 (Malignant) hypertension 0.59
4 Mesangiocapillary glomerulonephritis 0.17
5 FSGS 0.14
6 Membranous glomerulonephritis 0.03
7 IgM nephropathy 0.17
8 Microangiopathy 0.17
9 Focal segmental proliferative Gn 0.17
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.38
Secondary diagnoses and comments (if any):
Hypertension too*24. Interstitial nephritis too*4. ATN too *4. Consider
secondary causes*2. Crescent noted *2. Cholesterol embolus*2. Exclude
myeloma*1.
E.M.*8. Need to see IF*2. Congo red*1. EVG*1.
Original report and further information (if any):
Chronic ischaemic damage with superimposed IgA nephropathy
Circulation: U
Case number: 104 ....
Number of responses:40 . Date of analysis: 16 DEC 97
Clinical:
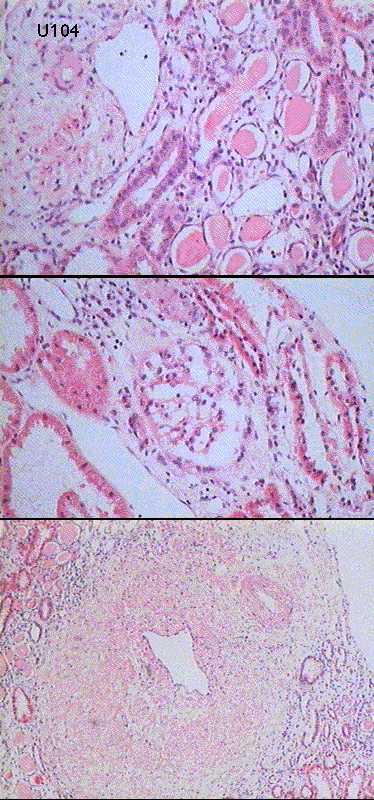
Previous ulcerative colitis. Renal impairment. Proteinuria. Recent
pregnancy - hypertension, decreased renal function, increased proteinuria.
Fetal death at 20 weeks gestation. Creatinine 157 umol/l IF negative. No
tissue for E.M.
Specimen:
H&E only
Diagnostic categories: Score:
1 Interstitial nephritis +/- infection 3.13
2 Infection / chronic pyelo. / reflux / scarring 2.05
3 Crystal / urate nephropathy 0.40
4 Don't know, can't tell, not diagnostic etc. 0.50
5 Microangiopathy/eclampsia etc. 0.90
6 FSGS 0.33
7 Hypertension / vascular disease 1.40
8 Acute tubular necrosis / tubular damage NOS 1.00
9 Myeloma 0.05
10 Developmental anomaly (?neurofibromatosis?) 0.25
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 3.13
Secondary diagnoses and comments (if any):
Insufficient/inadequate material*14. Hypertension too*3. ATN too*1. Renal
angiography*1. IVP*1. EM on reprocessed material*2. Drug history?*1.
Original report and further information (if any):
Initial suggestion chronic pyelonephritis. Subsequently found to have
dilated pelvicalyceal system, cortical thinning and reflux. Had suffered
recurrent6 UTIs as a child; symptoms had become worse during pregnancy.
Circulation: U
Case number: 105 ....
Number of responses:57 . Date of analysis: 16 DEC 97
Clinical:
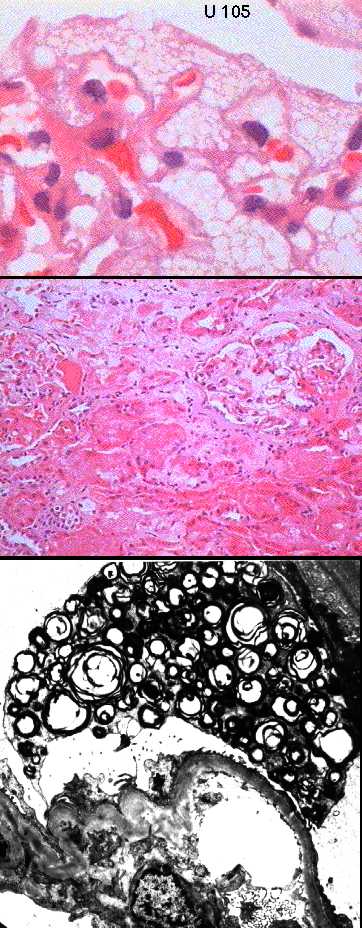
Male of 51 years, known diabetic, hepatitis B surface antigen positive.
Clinically, diabetic nephropathy unlikeley - no retinopathy. Haematuria and
proteinuria. Marked increase in serum IgA. IF negative.
Specimen:
H&E, E.M. prints*2.
Diagnostic categories: Score:
1 Fabry's disease 8.59
2 Focal segmental glomerulosclerosis 0.18
3 Lysosomal storage disease 0.18
4 Diabetic nephropathy 0.46
5 IgA nephropathy 0.04
6 Glomerulonephritis NOS 0.04
7 Toxic / drug induced damage 0.01
8 LCAT disease / lipid storage disorder 0.18
10 No diagnosis proffered 0.35
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.59
Secondary diagnoses and comments (if any):
Diabetic changes too*4. Check enzyme / alphagalactosidase levels*4.
Metabolic studies to exclude I - cell disease*1. Family history*2.
Angiokeratomas?*1.
Is this really selected within limits for an EQA case??*2.
Original report and further information (if any):
Fabry's disease
Circulation: U
Case number: 106 ....
Number of responses:58 . Date of analysis: 16 DEC 97
Clinical:
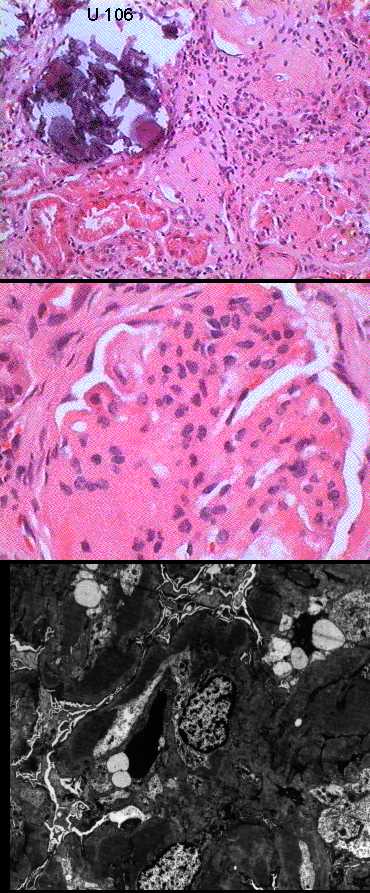
Short history of tiredness and lethargy with hypertension and weight loss in
male of 32 years. Found to be anaemic. IF: no glomeruli in sample.
Specimen:
H&E, E.M. prints *3
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis 6.53
2 Lupus nephritis 0.97
3 Proliferative /immune complex glomerulonephritis NOS 1.09
4 Membranous glomerulonephritis 0.48
5 FSGS 0.34
6 Proliferative glomerulonephritis ? IgA 0.22
7 Paraproteinaemia 0.02
8 AIDS nephropathy 0.17
10 No diagnosis proffered 0.17
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.53
Secondary diagnoses and comments (if any):
Nephrocalcinosis*18. Hypertension too*1.
Exclude SLE*5. Consider HIV*1. Hep.C?*1. Sarcoid?*1. Cryo?*2.
Immunoelectrophoresis*1.
Silver stain *8. PAS*3. Immunoperoxidase*11. Congo red *2. Better EM*2.
Original report and further information (if any):
Type I mesangiocapillary glomerulonephritis with much permanent renal
damage.
Circulation: U
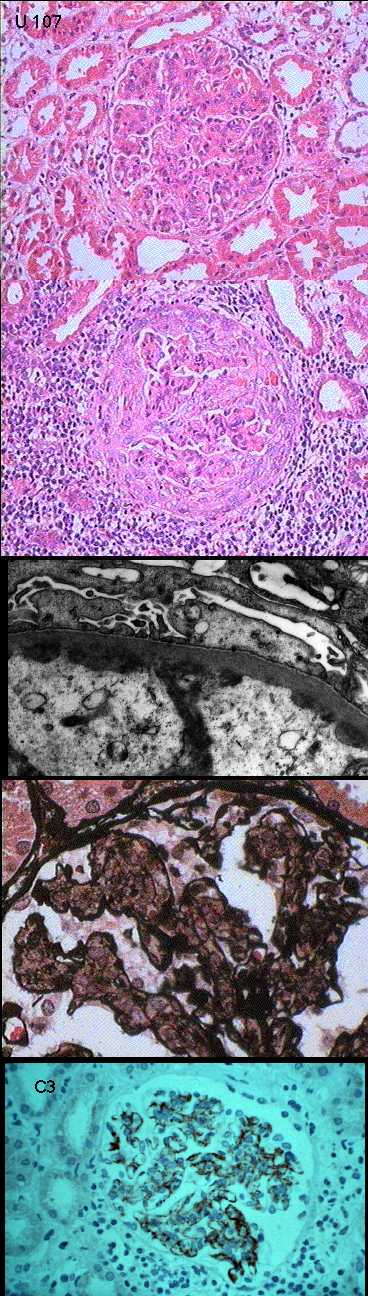
Case number: 107 ....
Number of responses:58 . Date of analysis: 16 DEC 97
Clinical:
Male, 27. Acute onset of proteinuria and haematuria. Albumin 27.
Creatinine 200 and rising daily. Hypertensive, BP 170/110. No oedema. ?
Acute nephritic syndrome ? cause. Immunoperoxidase: IgG and IgA look like
C3 (circulated) but with weaker staining. IgM negative.
Specimen:
H&E, Meth. AG, EM prints *2, IPx transparency of C3.
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis 4.86
2 Endocapillary / diffuse proliferative Gn. 3.21
3 Proliferative Gn / lupus nephritis 0.74
4 Microangiopathy 0.52
5 IgA nephropathy / Henoch Sch^nlein 0.38
6 Lupus nephritis 0.29
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.86
Secondary diagnoses and comments (if any):
Crescents noted*7. Exclude anti-GBM*1. Exclude SLE*2. Exclude IgA.
Exclude monoclonality in interstitial infiltrate *1. ASOT*3. C3 levels*1.
Original report and further information (if any):
Mesangiocapillary glomerulonephritis type 1.
Circulation: U
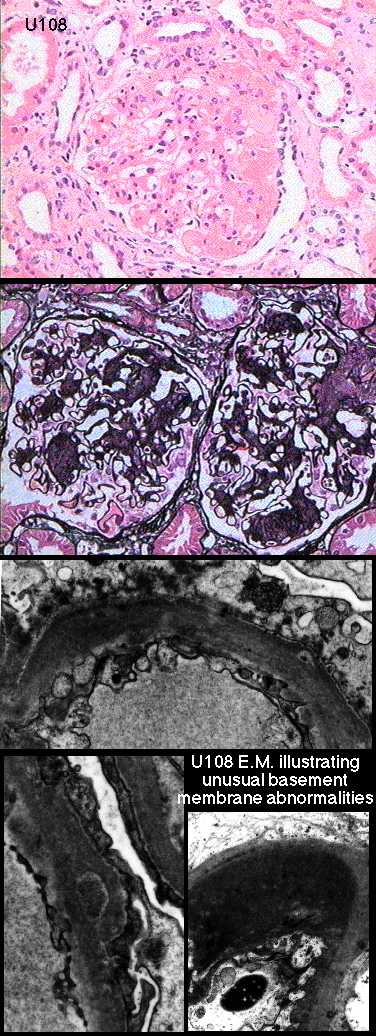
Case number: 108 ....
Number of responses:48 . Date of analysis: 16 DEC 97
Clinical:
47y.o. male. Nine years insulin dependent diabetes, with retinopathy.
Normotensive. 5g proteinuria. Normal creatinine. ANA+ve at 1:64. CRP1.5.
Diabetic nephropathy or something else? Immuno: Patchy IgM only, confined
to areas of glomerular sclerosis. FOR INTEREST & EDUCATION, NOT PERSONAL AS
Specimen:
H&E, Meth. silver, E.M. prints *3
Diagnostic categories: Score:
1 Diabetic nephropathy 8.21
2 Focal segmental glomerulosclerosis 0.58
3 Light chain nephropathy 0.31
4 Fibrillary glomerulonephritis 0.23
5 Lupus nephritis 0.33
6 Mesangial proliferative 0.31
7 Amyloid 0.02
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.21
Secondary diagnoses and comments (if any):
Comments on odd pattern of GBM damage *8. Deposits on EM ? significance *2.
E.M = fibrin cap?*1. Alport's disease *1. Consider HIV*2. ?amyloid*1.
Original report and further information (if any):
Original diagnosis: Diabetic nephropathy only. E.M. deposits attributed to
'sclerosis' & inspissated plasma proteins. GBM splitting & subepithelial
deposits not readily explained.
Links to cases in this document:
Top
U 103
U 104
U 105
U 106
U 107
U 108
 Home Page
Home Page
 CWIS
CWIS
 Pathology EQA
Pathology EQA
Last updated: 16 DEC 97
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582 Fax: (0116) 2584573
Email: pnf1@le.ac.uk