National Renal Pathology E.Q.A. Scheme
Circulation C
This document gives information on individual cases in
circulation C of this scheme. It contains no personal details
of participants.
Cases included:
C 152
C 153
C 154
C 155
C 156
C 157
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: C
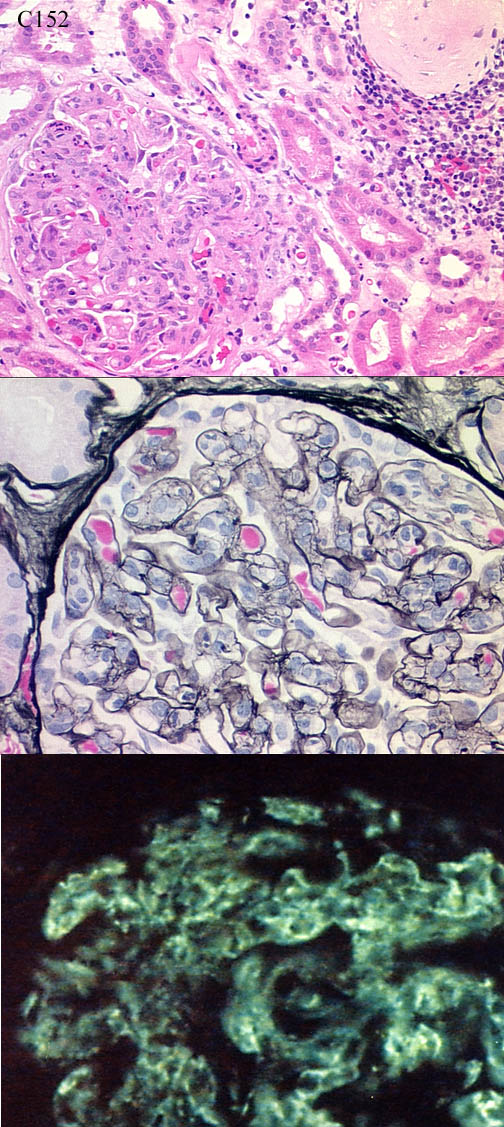
Case number: 152 ....
Number of responses:77 . Date of analysis: 10 SEP 00
Clinical:
67y.o. man, long history IHD. Recent onset ankle swelling with proteinuria
2g/24h. Creatinine 191 but falling to normal by time of biopsy. Cr
clearance 52, albumin 29, viscosity slightly raised. Smooth muscle
autoantibodies 1:160, others neg. C3 low, IgA slightly raised, C4, IgM, IgG
normal. No paraprotein. IF: C3 supplied, IgG similar but weaker, A&M
negative. No tissue for EM.
Specimen:
H&E, PAS, photo of IF for C3
Diagnostic categories: Score:
1 Post-strep./endocapillary/postinfective Gn 6.52
2 Mesangiocapillary / membranoproliferative Gn 3.18
3 Mesangial proliferative Gn 0.04
4 Diffuse proliferative Gn 0.26
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.52
Secondary diagnoses and comments (if any):
Atypical nephrotic presentation*1. EM*7. ASOT?*20. ANA/SLE?*7. ?SBE*1.
ATN too*1. IF for kappa & lambda*1. EM on paraffin material*2.
Original report and further information (if any):
Post-infective glomerulonephritis. Subsequently ASOT 1280 iu/ml and anti-
DNAase Ab 5720 iu/ml, i.e. recent post-streptococcal infection ? sinusitis.
Renal function subsequently returned to normal.
Circulation: C
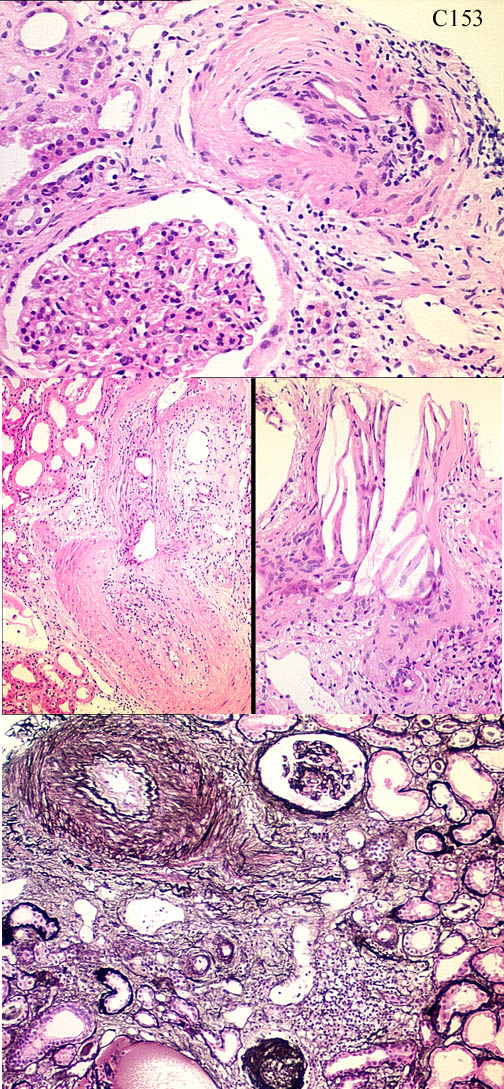
Case number: 153 ....
Number of responses:77 . Date of analysis: 10 SEP 00
Clinical:
Male, 62. renal failure developing over two months. IF for IgG, IgA, IgM,
C3 and fibrin all negative.
Specimen:
H&E, silver
Diagnostic categories: Score:
1 Cholesterol /atheromatous emboli 9.19
2 Hypertensive renovascular disease/atheroma 0.47
3 Vasculitis 0.01
4 Systemic sclerosis 0.19
5 Chronic thrombotic microangiopathy 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.19
Secondary diagnoses and comments (if any):
Exclude concurrent vasculitis*3. Glomerular changes ?2ry to emboli*1.
Angiography recently?*5. Aortic anurysm?*1. Hypertension*1. 2ry
interstitial nephritis*3. Exclude myeloma*1. Clinical info?*1.
Original report and further information (if any):
Cholesterol (atheromatous) embolisation and arteriosclerosis.Required
dialysis, but subsequently recovered renal function to creatinine 231umol.
Still has LVF and foot ulceration.
Circulation: C
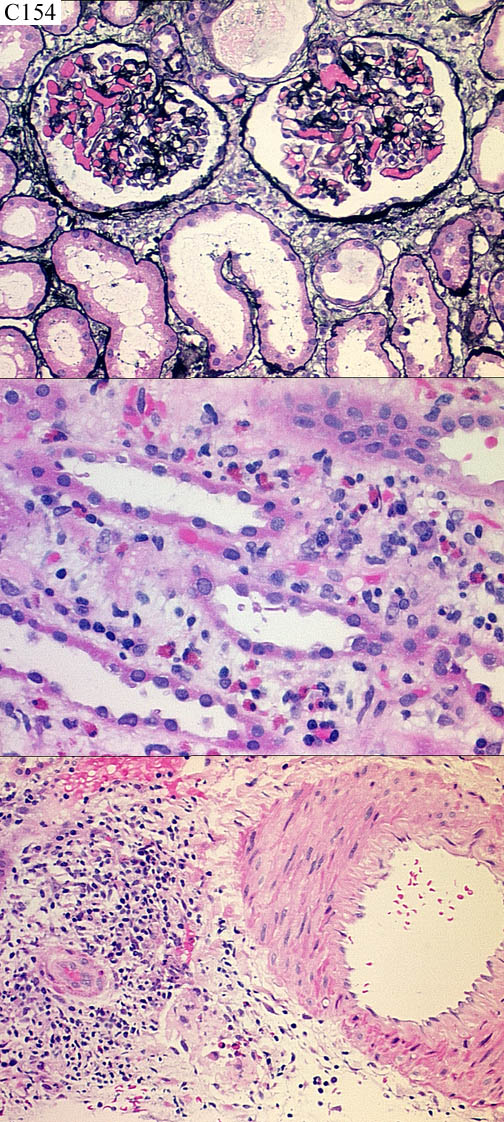
Case number: 154 ....
Number of responses:77 . Date of analysis: 10 SEP 00
Clinical:
Male, 41. Vomiting and haematemesis after big dose of paracetamol. Acute
hepatitis (Hep. B&C negative). Acute renal failure. Creatinine 377.
Enlarged kidneys - 13cm. IF: slight to moderage granular mesangial IgM and
C3; small amount of granular IgA, one glom. only. EM not contributory.
Specimen:
H&E, silver
Diagnostic categories: Score:
1 Acute interstitial nephritis 8.47
2 Acute tubular necrosis / hepatorenal syndr. 0.87
3 Renal vein thrombosis 0.13
4 Vasculitis 0.08
5 Interstitial nephritis & sickle cell disease 0.13
6 Hepatorenal syndrome 0.06
7 Microangiopathy +/- interstitial nephr. 0.26
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.47
Secondary diagnoses and comments (if any):
Eosinophils noted*18. Drug reaction?*33. ?ATN too*8. ?IgA nephropathy
underlying*3. ?renal vein thrombosis*4. DIC / coagulation in glomeruli?*
6. Hepatorenal syndrome*2. Thrombi in venules ? dehydration*1.
Original report and further information (if any):
'Acute' tubulo=interstitial nephritis, ? drug related. Also had hepatitis.
Both responded to steroid therapy; creatinine fell to 127umol.
Circulation: C
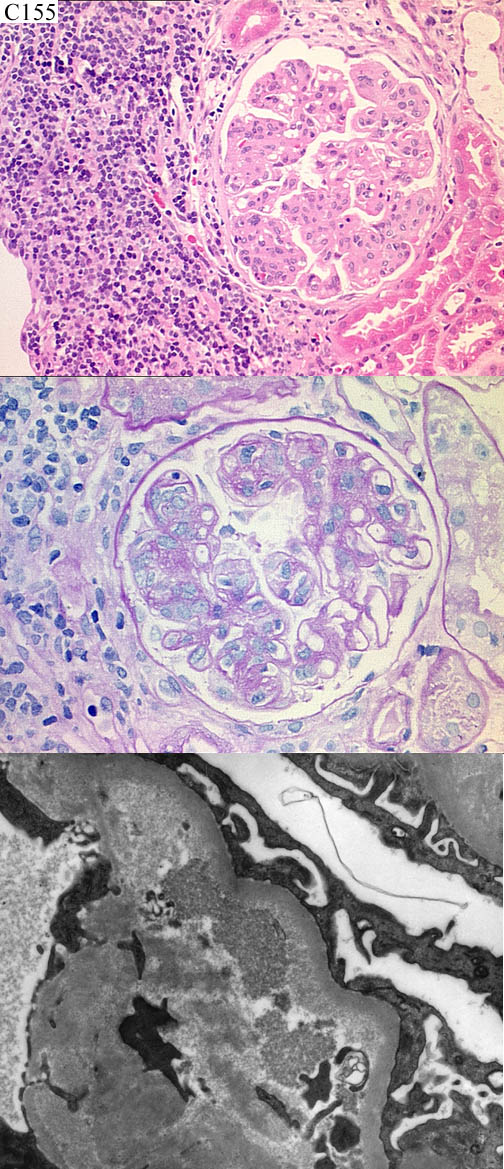
Case number: 155 ....
Number of responses:77 . Date of analysis: 10 SEP 00
Clinical:
68y.o. female. Low grade NHL 1984; relapse 1991, cleared by mild chemo.
Admitted for non-specific symptoms ??cirrhosis - LFTs normal. Lesions on
face - biopsy - confluent non-caseating granulomas (?elastolytic ?other
granulomatous disease) Creatinine 61 to 108 in 3 weeks, active urinary
sediment - renal biopsy. IF: patchy peripheral G, C3, C1q. M similar,
weaker. Lymphocytes mostly CD20+, scattered CD3. Kappa & lambda poor
quality, not informative.
Specimen:
H&E, PAS, silver, EM*3.
Diagnostic categories: Score:
1 Mesangiocapillary Gn 2.21
2 Mesangiocapillary Gn & (?) lymphoma infiltration 6.31
3 Fibrillary glomerulonephritis 0.13
4 Proliferative Gn AND lymphoma 0.26
5 Light chain nephropathy +/- lymphoma 0.97
6 Cryoglobulinaemia AND lymphoma infiltration 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.31
Secondary diagnoses and comments (if any):
Exclude cryoglobulinaemia*7. Exlude SLE*3. K&L immuno*7. Gene
rearrangements?*5. HepC status?*1. Congo red*2. Gn 2ry to lymphoma?*5.
Gn 2ry to chemotheapy?*2. Consider sarcoidosis*1.
Original report and further information (if any):
Mesangiocapillary pattern of glomerulonephritis in keeping with
cryoglobulinaemia. Lymphoid infiltrate suggestive of lymphoma.
Tumour was CD5+, CD23-, IgM kappa+ NHL. Bone marrow involvement.
Cryoglobulin IgG kappa 2g/l. Died 3 months after renal biopsy.
Circulation: C
Case number: 156 ....
Number of responses:77 . Date of analysis: 10 SEP 00
Clinical:
Nephrotic syndrome. C3 looked like IgG. IgM, IgA negative.
Specimen:
H&E, silver, EMx1, IgG projection slide x1.
Diagnostic categories: Score:
1 Membranous 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Age & sex of patient*2. Poor H&E*1. Poor silver*2.
Original report and further information (if any):
Membranous glomerulonephritis
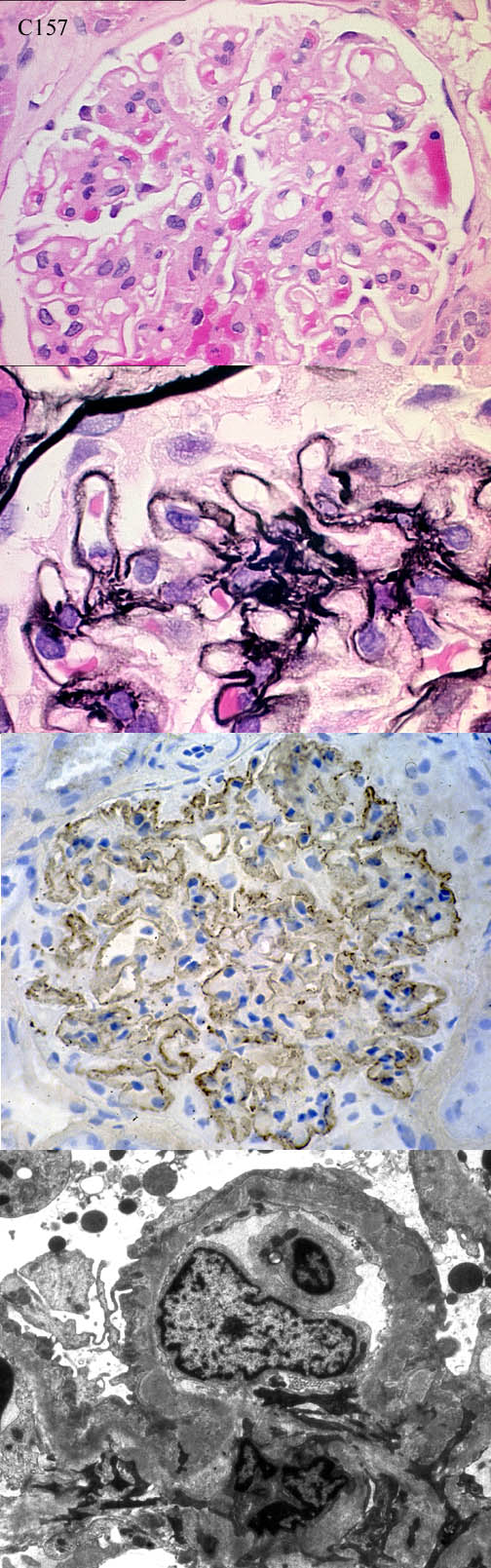
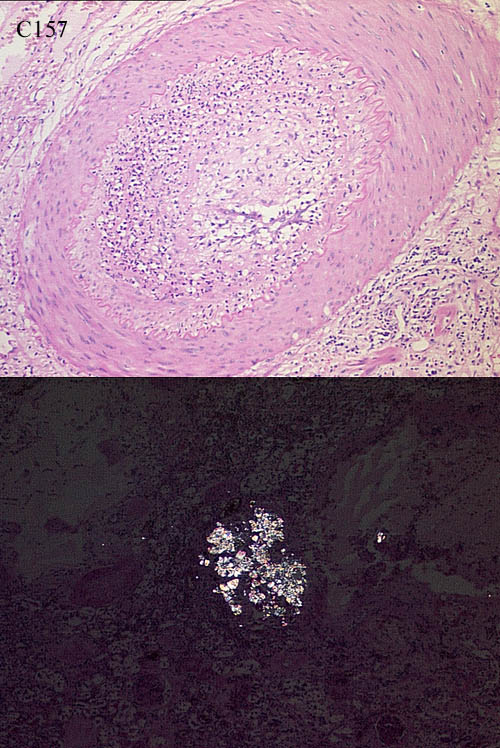
Circulation: C
Case number: 157 ....
Number of responses:51 . Date of analysis: 10 SEP 00
Clinical:
ODD CASE FOR INTEREST, NOT EQA. 37y.o. male, renal failure with acquired
cysts ? cause. Large bleed from ? renal carcinoma therefore nephrectomy.
No known bleeding diathesis. (Native kidney; NOT a transplant).
Specimen:
H&E
Macro:
Kidney 10x4.5cm. Multiple cysts up to 1cm. Parenchyma much reduced. Massive
maemorrhage into renal and pelvic tissues, including a haematoma 13cm. No
tumour seen.
Diagnostic categories: Score:
1 Vascular damage - from arterial embolisation? 0.41
2 Vasculitis 3.88
3 Vascular disease / chronic damage NOS 2.18
4 Post-biopsy/post haemorrhage vascular inflammation 0.49
5 Interstitial nephritis 0.24
6 Infection 0.65
7 Angiomyolipoma 0.29
8 A-V malformation 0.86
9 Scleroderma/hypertension 0.51
10 Crystal deposition (Oxalosis or gout) 0.49
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 3.88
Secondary diagnoses and comments (if any):
ANCA*2. Elastin*1. MSB*1. Kawasaki's disease?*1. Any vascular
abnormalities elsewhere?*1. Oxalate crystals noted *4. 'Crystal
granulomas'*1. Drug reaction?*1.
Other suggestions: Oncocytoma?*1. Leukaemic infiltrate?*1.
Original report and further information (if any):
Arteriovenous fistula with vascular changes of unknown significance. No
history of vascular embolisation before nephrectomy. Original cause of
renal failure was HUS, several years ago.
Links to cases in this document:
Top
C 152
C 153
C 154
C 155
C 156
C 157
Last updated: 10 SEP 00
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk