National Renal Pathology E.Q.A. Scheme
Circulation B
This document gives information on individual cases in
circulation B of this scheme. It contains no personal details
of participants.
Cases included:
B 146
B 147
B 148
B 149
B 150
B 151
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: B
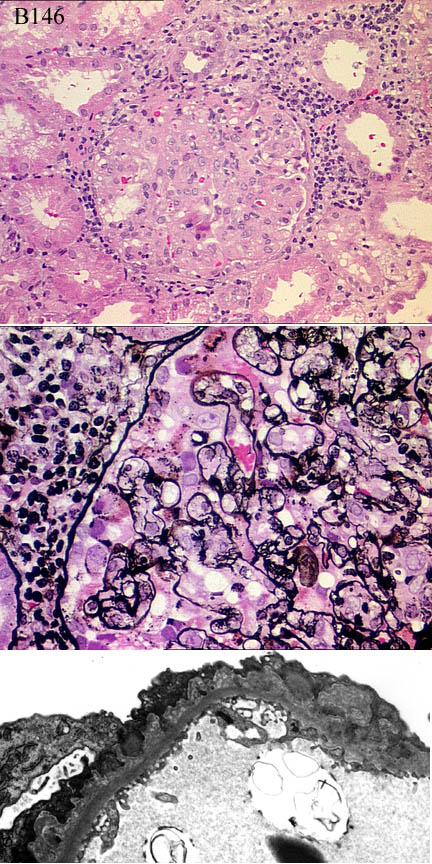
Case number: 146 ....
Number of responses:74 . Date of analysis: 10 SEP 00
Clinical:
12 y.o. girl, presented with nephrotic syndrome and haematuria. BP normal,
creatinine 70umol, lupus seology negative, C3c low, C4 normal, no extra-
renal manifestations, no improvement after steroids. IF: diffuse granular
IgG+++ along capillaries, weak C3c and IgM.
Specimen:
H&E, silver, EMx2
Diagnostic categories: Score:
1 Membranous 4.22
2 Membranoproliferative / mesangiocapillary Gn 1.82
3 Acute diffuse proliferative / post-infectious Gn 2.76
4 Alport syndrome 0.08
5 Lupus 0.72
6 Focal segmental glomerulonephritis 0.27
7 Mesangioproliferative gn 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.22
Secondary diagnoses and comments (if any):
Exclude lupus / lupus serology*12. Exclude 2ry membranous*4. Interstitial
changes - bad prognosis?*4. Crescent?*7. Exclude Alports*1.
Insufficient material for diagnosis*3. ASOT*6. EM & light don't match*6.
Several participants gave lengthy discussions.
Original report and further information (if any):
Membranous pattern with proliferation, reported as membranoproliferative
glomerulonephritis with subepithelial deposits. No response to
prednisilone & CyA. |Some improvement after cyclophosphamide. C3 nephritic
factor reported as '69% of pool i.e. below normal range' (???).
Circulation: B
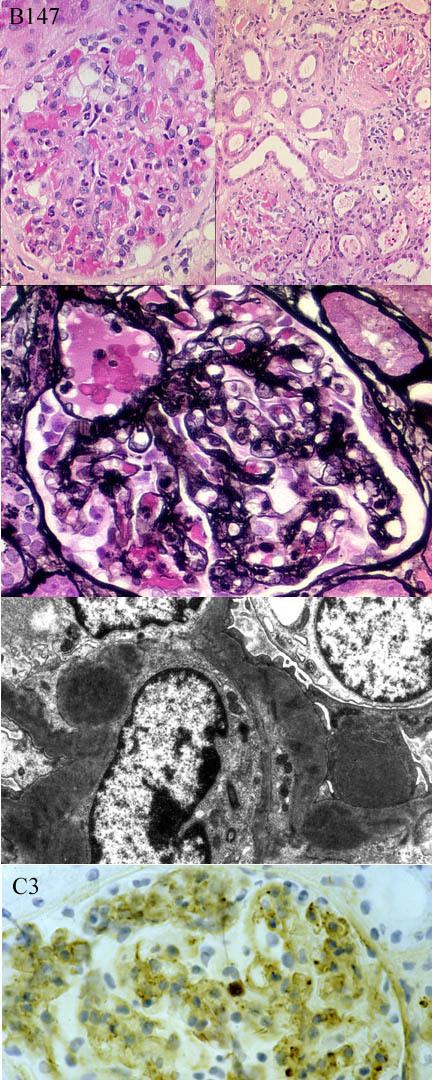
Case number: 147 ....
Number of responses:73 . Date of analysis: 10 SEP 00
Clinical:
Female, 70y.o. Admitted with cough, pleural effusion, epistaxis, urea 17,
creatinine 310, Cr clearance 15ml/min, 1.33g proteinuria/24h. Elevated ASOT
(800iu/ml) and anti-DNAase beta (1600). Immuno: C3 circulated, C1q and
heavy chains negative
Specimen:
H&E, PAMS, EMx1, C3 projection slide
Diagnostic categories: Score:
1 Post strep /acute diffuse /endocapillary Gn 9.15
2 Focal proliferative Gn NOS 0.21
3 Mesangiocapillary / membranoproliferative Gn 0.16
4 Lupus nephritis 0.30
5 Mesangial proliferative Gn 0.14
6 Cryoglobulinaemia 0.04
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.15
Secondary diagnoses and comments (if any):
Exclude microangiopathy/vasculitis*2. Exclude cryoglobulin *2. Exclude
lupus*1. Biopsy late in course*1. Need other IF*1.
Original report and further information (if any):
Post-streptococcal glomerulonephritis. The lack of IgG with mesangial C3
suggests that the process is resolving.
Circulation: B
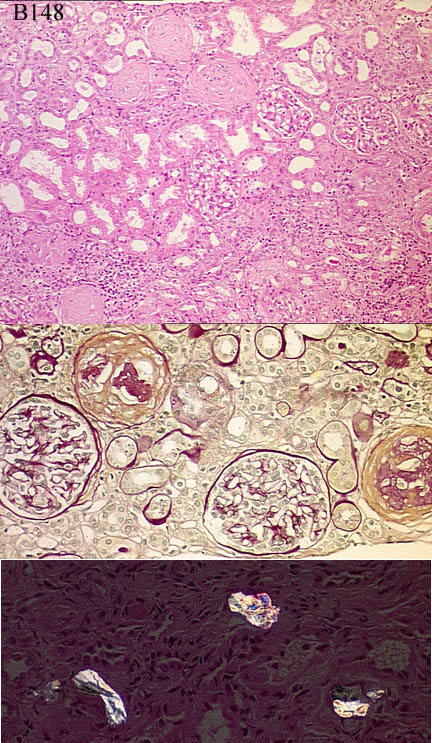
Case number: 148 ....
Number of responses:73 . Date of analysis: 10 SEP 00
Clinical:
Female aged 75. Renal faiure (creatinine 540). Past history of gastric
lymphoma. Proteinuria 0.2g. Normal kidney on ultrasound. IF: IgA++, C3++,
IgM+, all mesangial.
Specimen:
H&E, PAS, silver
Diagnostic categories: Score:
1 IgA nephropathy+/- interstitial nephritis 8.95
2 Scarring NOS, possibly IgA related 0.16
3 IgA and ? lymphoma 0.14
4 Immunotactoid glomerulopathy 0.14
5 Interstitial nephritis & oxalosis 0.14
6 Cryoglobulinaemia 0.14
7 Mesangiocapillary Gn 0.14
8 Light chain nephropathy 0.07
9 Interstitial nephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.95
Secondary diagnoses and comments (if any):
ATN too*4. Exclude lymphoma*12. IgA 2ry to intestinal disease?*7. IgA
2ry to maltoma*2. Is IgA monoclonal?*1. . EM*3. LFTs*1. More clinical
info*1. Any radiotherapy to kidney?*1. More IF*2. Pale H&E*3. Poor
silver*3. Unsuitable for EQA*5.
Original report and further information (if any):
Circulation: B
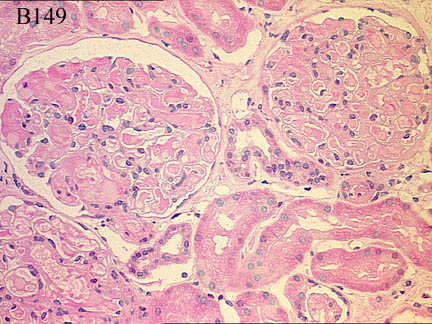
Case number: 149 ....
Number of responses:73 . Date of analysis: 10 SEP 00
Clinical:
74 year old man, presented with anaemia, haematurai and proteinuria.
Creatinine 143, urea 7,3, renal ultrasound normal. Serological evidence of
Waldenstrom's macroglobulinaemia.
Specimen:
H&E
Diagnostic categories: Score:
1 Cryoglobulinaemia / Waldenstrom's 9.16
2 Possible cryo, material not diagnostic 0.14
3 Hyaline thrombi 0.29
4 Fibrillary glomerulopathy 0.14
10 Inadequate material, no diagnosis offered 0.27
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.16
Secondary diagnoses and comments (if any):
Silver*7. Immuno *11. EM*4. PAS*11. MSB*2. Congo red*5. H&E too pale*5.
Exclude amyloid*5. Unsuitable for EQA*2.
Original report and further information (if any):
Non-cryoglobulinaemic glomerular / small vessel involvement with
Waldenstrom's macroglobulinaemia.
Circulation: B
Case number: 150 ....
Number of responses:73 . Date of analysis: 10 SEP 00
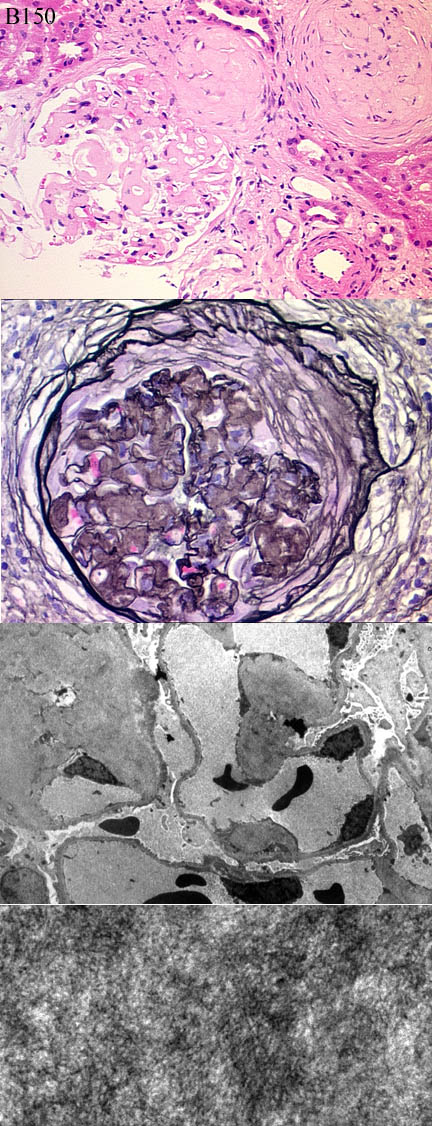
Clinical:
64 year old woman. nephrotic, proteinuria 5g and albumin 32g/l. Creatinine
normal (78), Cr. cleaeance 83ml/min. IgG kappa paraprotein 3.34g/l. Ig
levels normal. Bone marrow: 7% plasma cells, 40% abnormal lymphocytes. No
free light chains. Raised viscosity. ANA weak at 1:80, other autoantibodies
negative. Amyloid stains and IF negative.
Specimen:
H&E, PAS, EM*1.
Diagnostic categories: Score:
1 Amyloidosis 3.03
2 Fibrillary Gn 2.64
3 Monoclonal immunoglobulin deposition disease 1.64
4 Light chain disease (Merge with 3?) 2.17
5 Immunotactoid glomerulopathy 0.25
6 Non-amyloid fibrillar glomeruopathy, NOT fibrillary Gn 0.27
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 3.03
Secondary diagnoses and comments (if any):
'PAS' section is actually a silver - *many. Repeat Congo red*10. Repeat
IF*3. Fibronectin deposits?*1. Amyloid A & P immuno*2. Scale on EM*2.
Higher mag/better EM*2. Kappa & lambda immuno*9. ? lymphomatous
infiltrate*3. Better clinical info*2.
Unsuitable for EQA*3.
Original report and further information (if any):
Fibrillary glomerulonephritis??? Peripheral blood lymphocytes not
monoclonal, no diagnosis of myeloma or lymphoma. paraprotein level remains
stable. Renal function slowly deteriorating. Heavy proteinuria (5g)
persists.
Circulation: B
Case number: 151 ....
Number of responses:63 . Date of analysis: 10 SEP 00
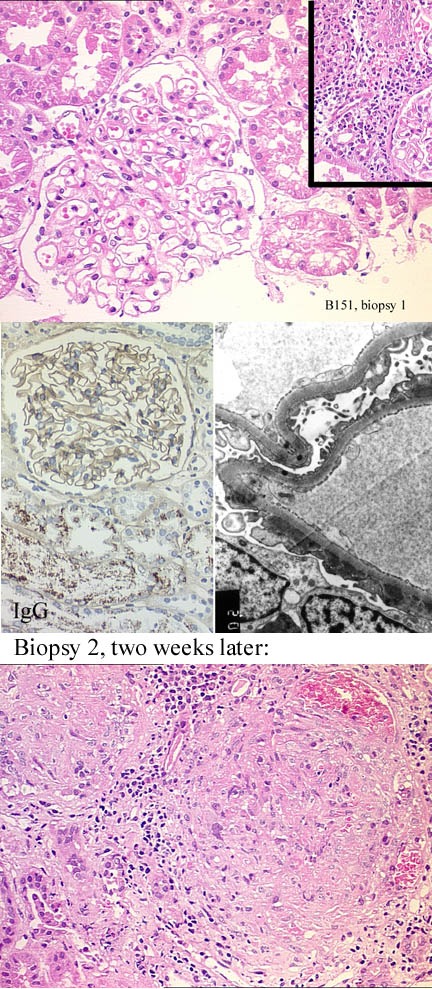
Clinical:
Male, 29, no past history. Presented overtly nephrotic with normal serum
creatinine; Biopsy 1 performed. Re-presented 2 weeks later with acute
renal failure; biopsy 2 performed. Serum anti-GBM then found to be
positive. CASE FOR INTEREST & EDUCATION, NOT EQA.
Specimen:
Bx 1: H&E, EM&IgG. Bx2: H&E only
Diagnostic categories: Score:
1 Membranous Gn THEN Goodpasture's 7.30
2 Goodpastures only mentioned 1.59
3 Membranous only mentioned 0.48
4 Post-infective Gn then Goodpasture's 0.32
5 Immune complex Gn NOS 0.16
6 Granulomatous glomerulonephritis 0.16
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.30
Secondary diagnoses and comments (if any):
ANCA?*1. Why not for scoring?*1.
Original report and further information (if any):
Presentation with membranous Gn, subsequent development of Goodpasture's.
Has the membranous damage 'unmasked' the Goodpasture epitope? MEDLINE
search; 3 case reports of 'simultaneous' membranous & Goodpasture's, none
sequential.
Links to cases in this document:
Top
B 146
B 147
B 148
B 149
B 150
B 151
Last updated: 10 SEP 00
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk