National Renal Pathology E.Q.A. Scheme
Circulation A
This document gives information on individual cases in
circulation A of this scheme. It contains no personal details
of participants.
Cases included:
A 140
A 141
A 142
A 143
A 144
A 145
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: A
Case number: 140 ....
Number of responses:75 . Date of analysis: 10 JAN 00
Clinical:
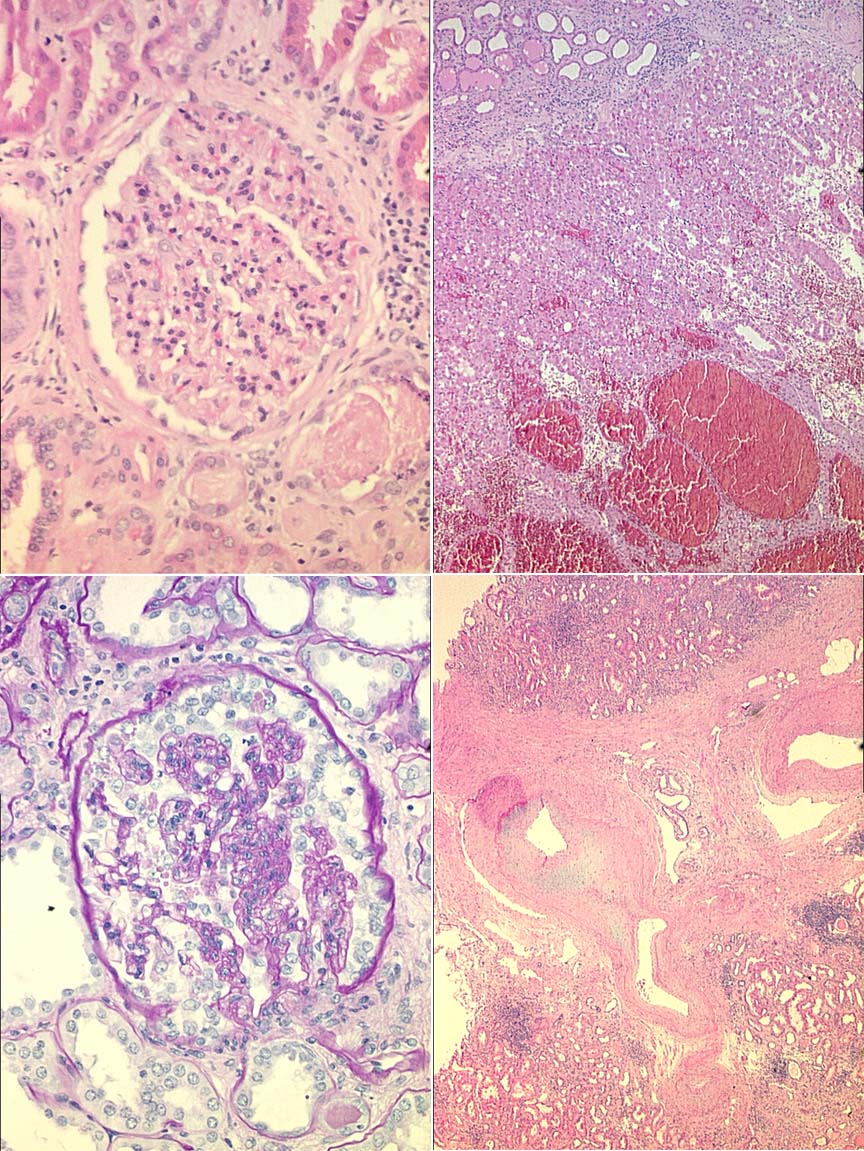
55y.o. with polycystic kidney disease. Tumour mass 4x3x3cm, homogenous cut
surface with areas of haemorrhage. Patient also had proteinuria 8g/24h
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Renal cell carcinoma (+/- 'granular cell' or 'oncocytic'1.91
2 Renal cell carcinoma and minimal change/FSGS/other Gn 1.51
3 Oncocytoma 3.20
4 RCC and segmental glomerulosclerosis ? overload 0.13
5 Collecting duct carcinoma 0.23
6 Oncocytoma and minimal change/FSGS/other Gn 2.75
7 FSGS (tumour not mentioned) 0.13
8 Oncocytoma + myeloma / cast nephropathy 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 3.20
Secondary diagnoses and comments (if any):
Cause of 8g proteinuria needs immuno + EM to sort out*15. Better gross
description*6. More blocks to exclude RCC*11. Cytogenetics*1. Silver
stain*1. Congo red*4. Hale's colloidal iron*5. Hypertension/scarring
too*12. Seg. sclerosis-1ry or 2ry to hypertension?*4. Exclude diabetes*2.
Separate tiny papillary adenoma*2. Why so few cysts?*3. Renal vein
thrombosis?*1. Unsuitable for EQA*1.
Original report and further information (if any):
Circulation: A
Case number: 141 ....
Number of responses:75 . Date of analysis: 10 JAN 00
Clinical:
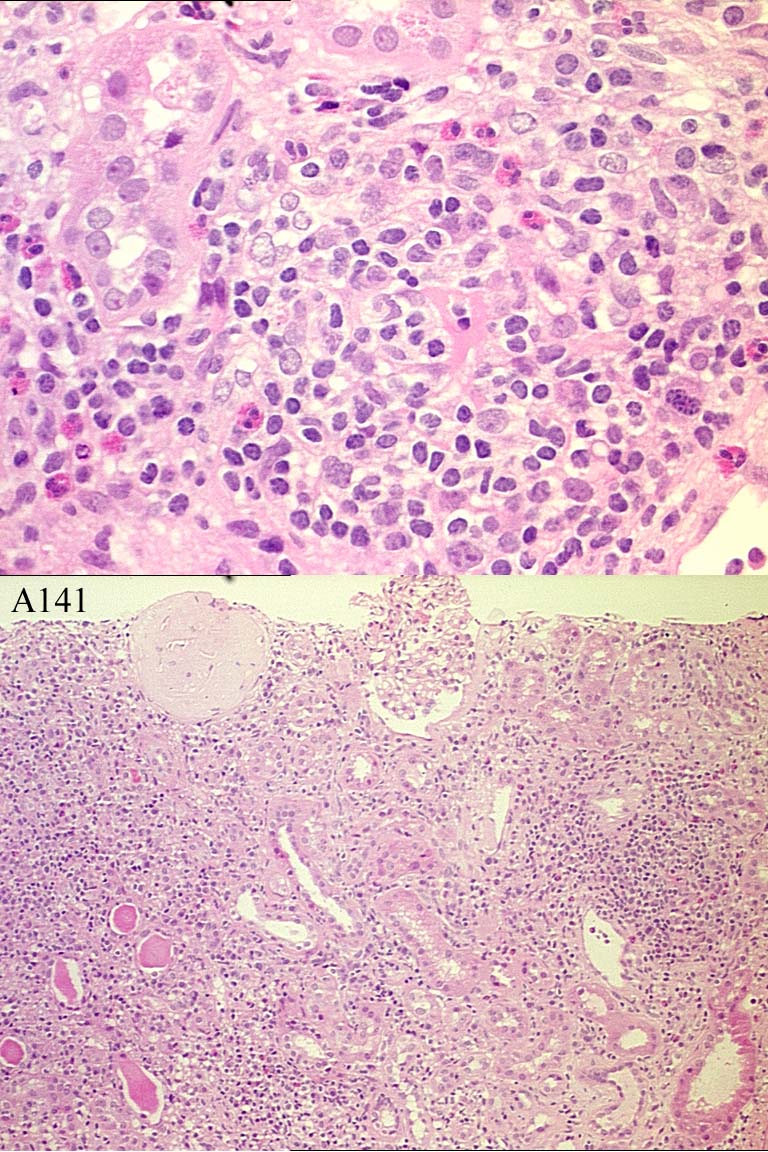
66y.o female, 6/12 hx joint pains & vague symptoms. On Didronel for
osteoporosis. Intermittent Voltarol. Elevated rheumatoid factor, negative
ANCA, deteriorating renal function (urea 25, creat. 397). Calcium low
normal. IF negative. EM not done.
Specimen:
H&E only
Diagnostic categories: Score:
1 Interstitial nephritis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Drug related?*36. Allergic?*3. Auto-immune/RhA?*2. EM*1. Lymphoma??*1.
Storage disorder??*1. Whipple's??*1. ATN too*1. Eaten wild mushrooms?*1.
Congo red*1. Exclude myeloma*1. Pale H&E*7.
Original report and further information (if any):
Circulation: A
Case number: 142 ....
Number of responses:75 . Date of analysis: 10 JAN 00
Clinical:
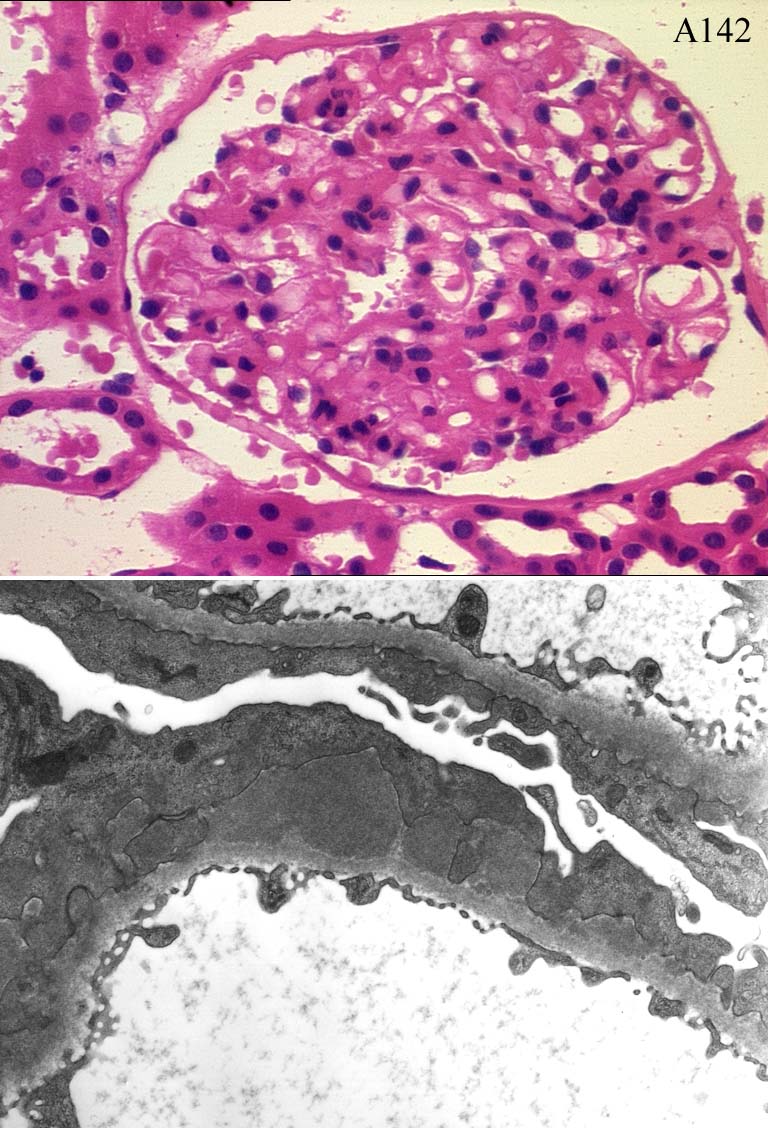
57y.o. female. Presented with nephrotic syndrome. Urinary protein 10g/day.
Rheumatoid arthritis, recent penicillamine treatment. IF showed strong
capillary loop staining for IgG and C3.
Specimen:
H&E, EM x2
Diagnostic categories: Score:
1 Membranous Gn, penicillamine related 4.67
2 Membranous Gn, penicillamine not mentioned 5.33
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 5.33
Secondary diagnoses and comments (if any):
Silver stain*3. How long on penicillamine?*1.
Original report and further information (if any):
Circulation: A
Case number: 143 ....
Number of responses:75 . Date of analysis: 10 JAN 00
Clinical:
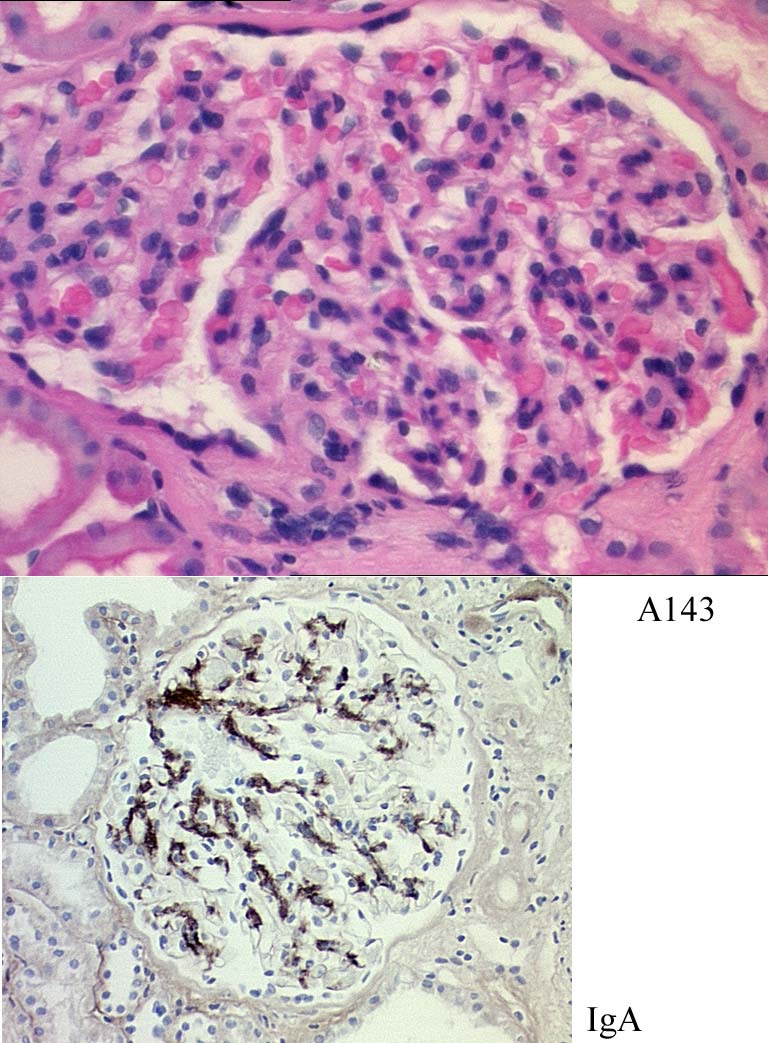
Male, 29. At age 17, clinical diagnosis Henoch Schonlein purpura, no biopsy.
Age 25; purpuric rash, haematuria, proteinuria. On treatment for
hypertension since then. Now well, but haematuria & proteinuria 2.33g/24h.
No immunological abnormality in serum. No IgG on IPx.
Specimen:
H&E, IPx for IgA
Diagnostic categories: Score:
1 IgA nephropathy / HSP 9.87
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.87
Secondary diagnoses and comments (if any):
Hypertension too*3. Silver*1. Thick H&E*2.
Original report and further information (if any):
Circulation: A
Case number: 144 ....
Number of responses:75 . Date of analysis: 10 JAN 00
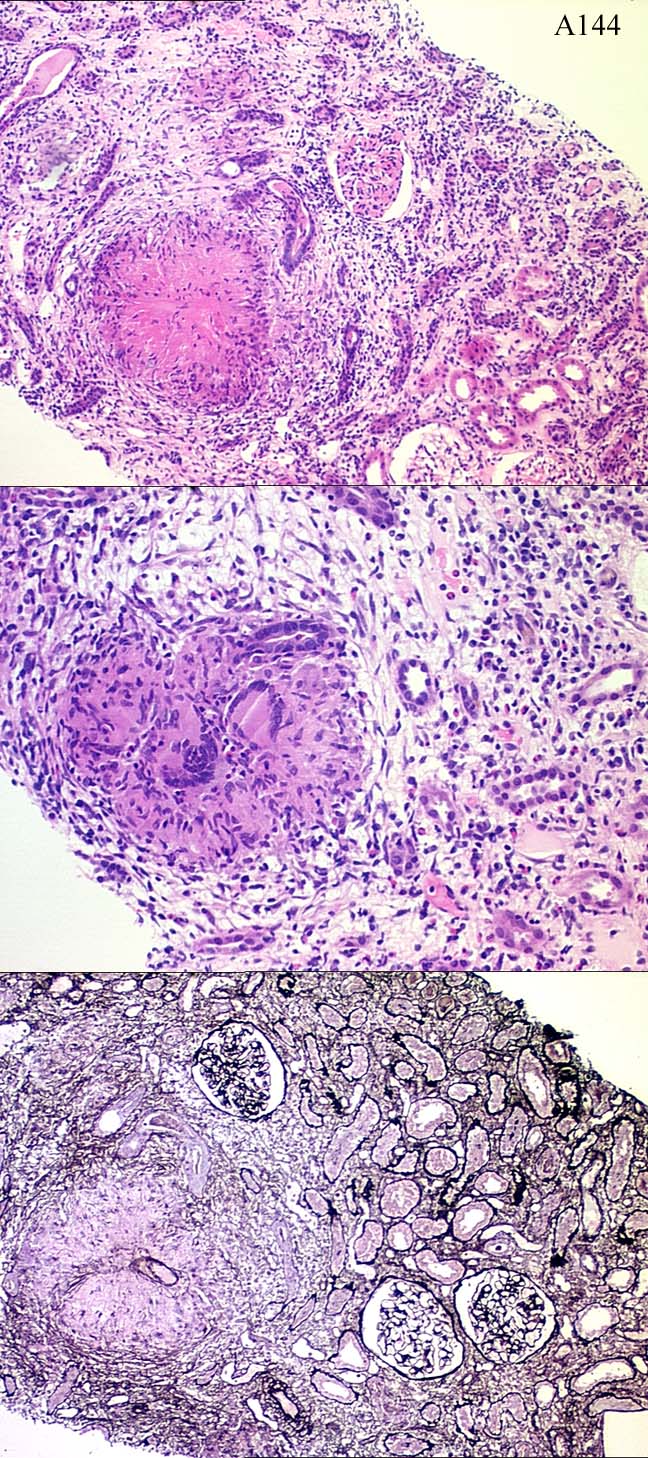
Clinical:
40 y.o. Maltese female, creatinine 161, recent E coli UTI, proteinuria 0.
4g/day, normal BP, negative ANF, ESR 140, CRP 105 IF: IgM and C3 in small
vessels; glomeruli negative.
Specimen:
H&E, silver
Diagnostic categories: Score:
1 Granulomatous T - I nephritis NOS 1.33
2 Granulomatous TIN differential given 4.67
3 Granulomatous TIN probably sarcoid 0.27
4 Granulomatous TIN probably TB 1.73
5 Granulomatous TIN probably Wegener's 1.33
6 Granulomatous TIN probably drug induced 0.53
7 Granulomatous TIN, probably chronic UTI 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 4.67
Secondary diagnoses and comments (if any):
?TB*50, ?drug reaction*23, ?fungi?13, ?sarcoid*19, ?Wegener's*18, ?Churg
Strauss*4, ?Brucella*6, ?viral*1, ?E coli*5, ?parasites*1. ?Crohn's*1.
EVG*1. PAS-D*4. MSB*1. EM*1. Von Kossa*1. Urine culture*4.
Original report and further information (if any):
Granulomatous vasculitis and necrotising glomerulitis; differential
includes Wegener's, necrotising sarcoid and Churg-Strauss syndrome. Not
TB. Subsequently, ANCA found positive and patient revealed URT symptoms;
diagnosis Wegener's.
Circulation: A
Case number: 145 ....
Number of responses:73 . Date of analysis: 10 JAN 00
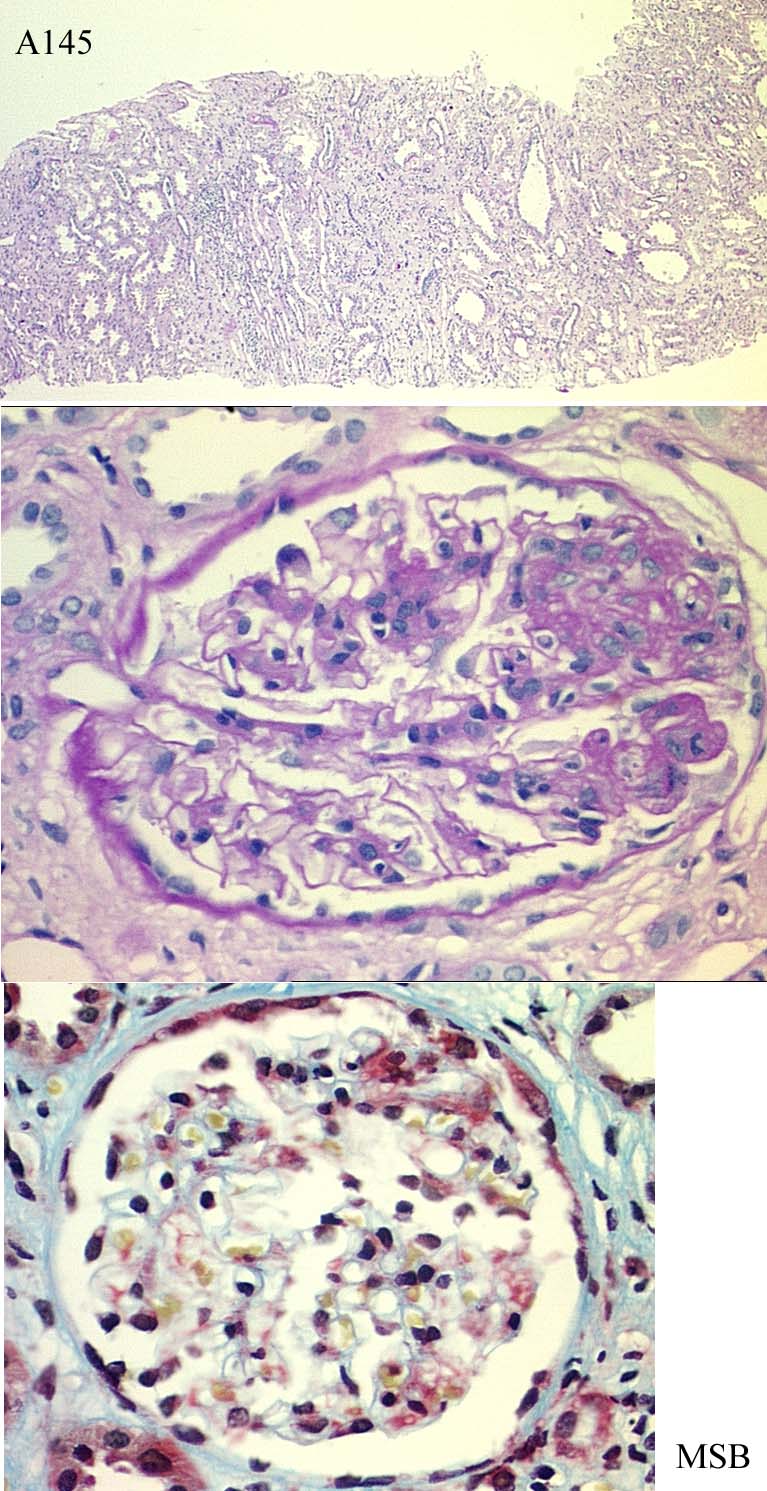
Clinical:
12 year old boy. Cryptogenic cirrhosis. Liver transplant 5 years ago.
Cyclosporin treatment for 3 years >5mg/kg then switched to microphenalin.
Declining renal function.
Specimen:
PAS, MSB (H&E not submitted)
Diagnostic categories: Score:
1 Cyclosporin toxicity 6.60
2 Interstitial & glomerular fibrosis ? cause 0.32
3 Focal glomerulonephritis/glomerulosclerosis NOS 0.81
4 Nodular glomerulosclerosis 0.07
5 TTP/HUS 0.42
6 Transplant glomerulopathy 0.00
7 FSGS 1.64
10 Transplant case so diagnosis not offered 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.60
Secondary diagnoses and comments (if any):
Immuno.*3. EM*2. Silver*1. Fibrosis related to cirrhosis?*2. IgA?*1. HIV
status?*1. Microangiopathy due to CyA?*3. CyA levels?*1. Unsuitable for
EQA*2. What is microphenelin*many? - (Presumably means mycophenolate
mofetil . I just copied the spelling! - PF)
Original report and further information (if any):
Links to cases in this document:
Top
A 140
A 141
A 142
A 143
A 144
A 145
Last updated: 10 JAN 00
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk