National Renal Pathology E.Q.A. Scheme
Circulation N
This document gives information on individual cases in
circulation N of this scheme. It contains no personal details
of participants.
Cases included:
N 212
N 213
N 214
N 215
N 216
N 217
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: N
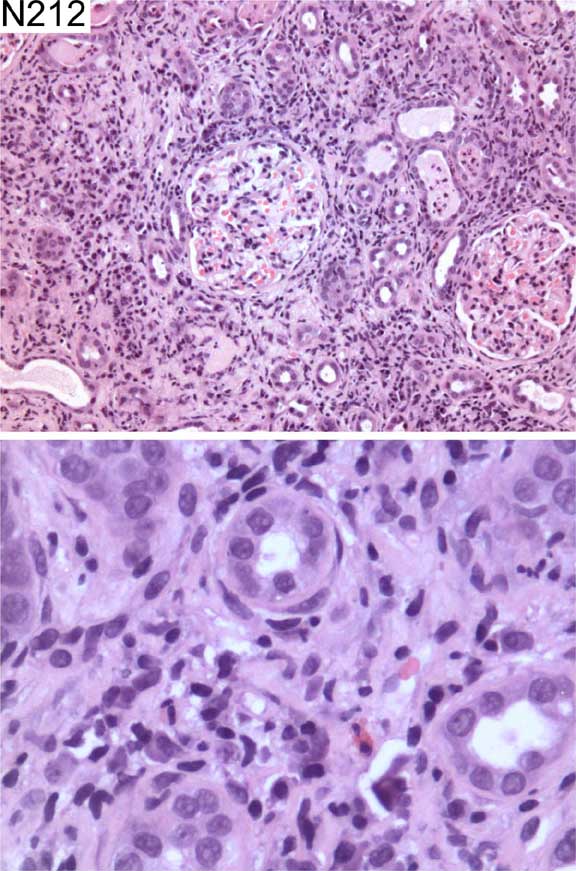
Case number: 212
....
Number of responses:82 . Date of analysis: 28 DEC 03
Clinical:
Female, 64 y.o. Sweating, high ESR (126mm/hr), polyuria, polydipsia, ANCA
negative. CRP<6, creatinine 250.
Specimen:
H & E
Diagnostic categories: Score:
1 Acute interstitial nephritis (exclude infection) 4.27
2 Interstitial nephritis (NOS) 2.95
3 Myeloma 0.24
4 Acute interstitial nephritis 1.34
5 Chronic interstitial nephritis 0.49
6 Interstitial nephritis suspicious of myeloma 0.37
7 Pyelonephritis 0.22
8 Interstitial nephritis secondary to pyelonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.27
Secondary diagnoses and comments (if any):
Immuno*4. EM*1. Exclude myeloma (cast nephropathy)*14. Excludy lymphoma (
atypical cells)*2. Congo red*1. Exclude drug/allergic reaction*19.
Consider sarcoid*1. Uveitis?*2. Diabetes insipidus?*1. Diabetes mellitus?*
2. Lupus serology?*1. Lupus anticoagulant?*1. Viral infection?*1.
Original report and further information (if any):
Circulation: N
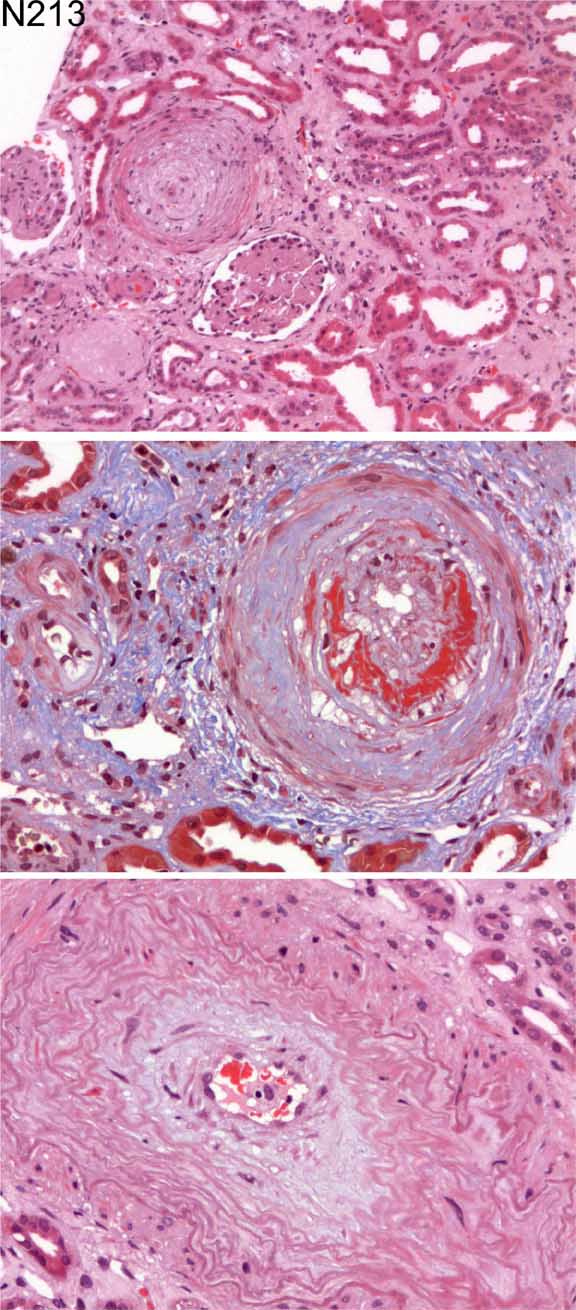
Case number: 213
....
Number of responses:82 . Date of analysis: 28 DEC 03
Clinical:
Female, 74 yrs. Acute renal failure ?cause (probably secondary to sepsis).
ANA 1:320 (speckled), ANCA, anti-GBM negative. Decreased immunoglobulins on
serum electrophoresis. Clinical signs of systemic sclerosis but not
hypertensive. Treated with inotropes for hypotension and subsequently
improved. Subsequent enquiry: she became acutely hypertensive, following
admin of steroids at another hospital, went into ARF. Had definite clin
diagnosis of scleroderma. She remains dialysis dependent.
Specimen:
H & E, MSB
Diagnostic categories: Score:
1 Vasculopathy c/w systemic sclerosis 9.76
2 Small vessel vasculopathy 0.12
3 Vasculopathy secondary to hypertension 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.76
Secondary diagnoses and comments (if any):
PAS*1. Silver*2. Fibrin stain*1. Changes induced by steroids for PSS?*1.
Serology*2. IF*2. BP?*2. Timing of biopsy in relation to history?*1.
Original report and further information (if any):
Circulation: N
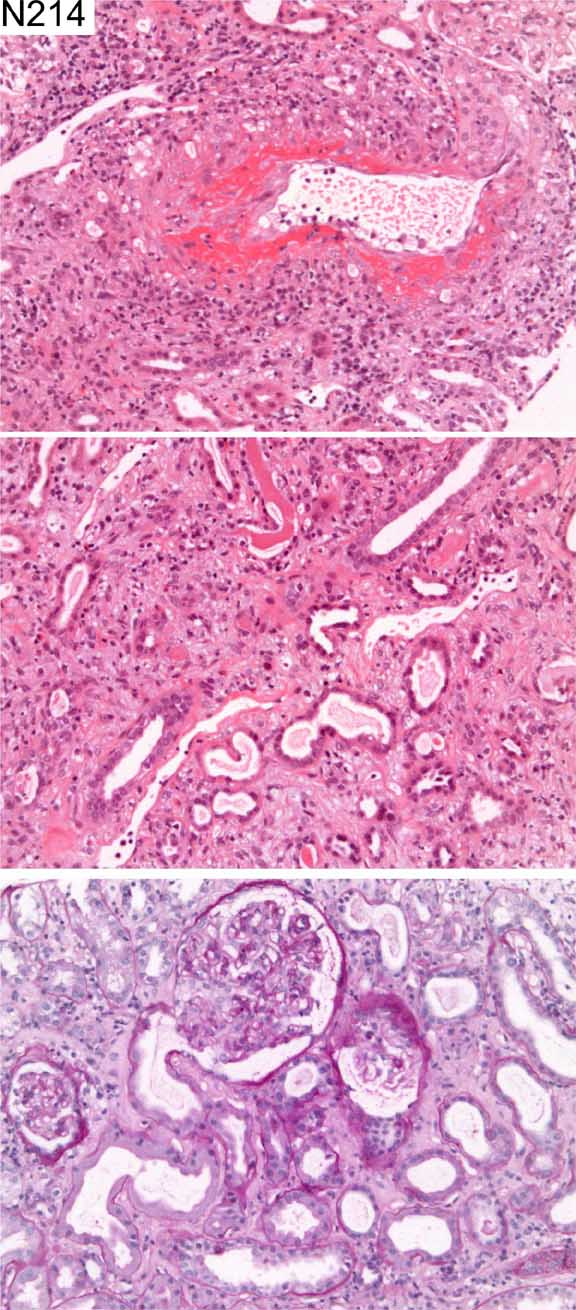
Case number: 214
....
Number of responses:82 . Date of analysis: 28 DEC 03
Clinical:
Female, 62 yrs. Sudden onset of deafness, pulmonary opacity noted on CXR,
haematuria and proteinuria at presentation. Renal function normal. ANCA
positive. Immunofluorescence deposition of C3 and IgG in areas of fibrinoid
necrosis, otherwise negative.
Specimen:
H & E, PAS
Diagnostic categories: Score:
1 Vasculitic process, probably microscopic polyangiitis 2.85
2 Vasculitic process, probably Wegener's 4.71
3 Vasculitis NOS 2.44
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 4.71
Secondary diagnoses and comments (if any):
Eosinophils noted*1. Churg-Strauss?*2. Type of ANCA?*12. Lupus serology?*
1. BP?*1. CXR*1. Exclude infective endocarditis*1.
Original report and further information (if any):
Circulation: N
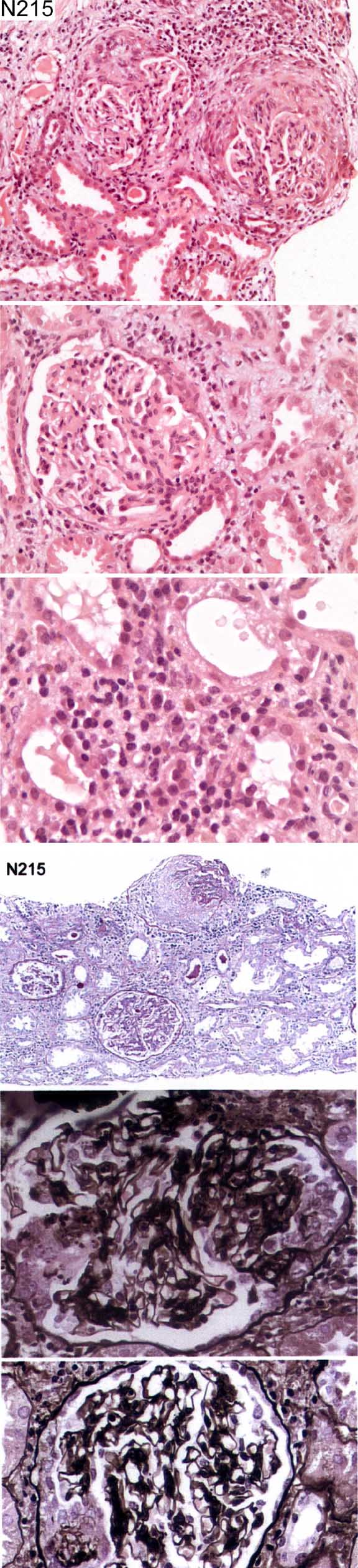
Case number: 215
....
Number of responses:82 . Date of analysis: 28 DEC 03
Clinical:
Female, 19yrs. Pre-eclampsic. Normal renal function post partum. Now
unwell with diarrhoea, vomiting, abnormal clotting, lethargy, frank
haematuria, proteinuria, creatinine 200.
Specimen:
H & E, photos of PAS and silver
Diagnostic categories: Score:
1 Crescentic glomerulonephritis NOS 6.63
2 Focal segmental glomerulosclerosis 0.24
3 Focal segmental glomerulonephritis 0.78
4 Crescentic Gn due to post-partum HUS 0.89
5 Post-partum thrombotic microangiopathy 0.37
6 Regenerating ATN 0.16
7 Eclampsia / Pre-eclampsia 0.37
8 IgA nephropathy / HSP 0.12
9 HUS-associated thrombotic microangiopathy 0.32
10 Thrombotic microangiopathy due to TTP 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.63
Secondary diagnoses and comments (if any):
EM*17. Immuno.*36. Anti-GBM antibodies?*4. Exclude HUS/TTP*8. Lupus
serology*14. Antiphospholipid?*1. ANCA*15. UTI?*1. Platelets?*1. Blood
film?*2. Tubulointerstitial nephritis*3. Clinically HELLP syndrome?*2. How
long post-partum?*3. Post-strep?*3. Need more information for definitive
diagnosis*17. Inadequate for EQA*18.
Original report and further information (if any):
Pauci-immune focal segmental necrotising glomerulonephritis of uncertain
aetiology. Patient was ANCA negative, autoantibodies negative (including
anti-GBM). Hep. B and C were negative. EM (done later) showed fibrin in
glomeruli but no convincing immune complex deposits. No follow-up
recorded.
Circulation: N
Case number: 216
....
Number of responses:82 . Date of analysis: 28 DEC 03
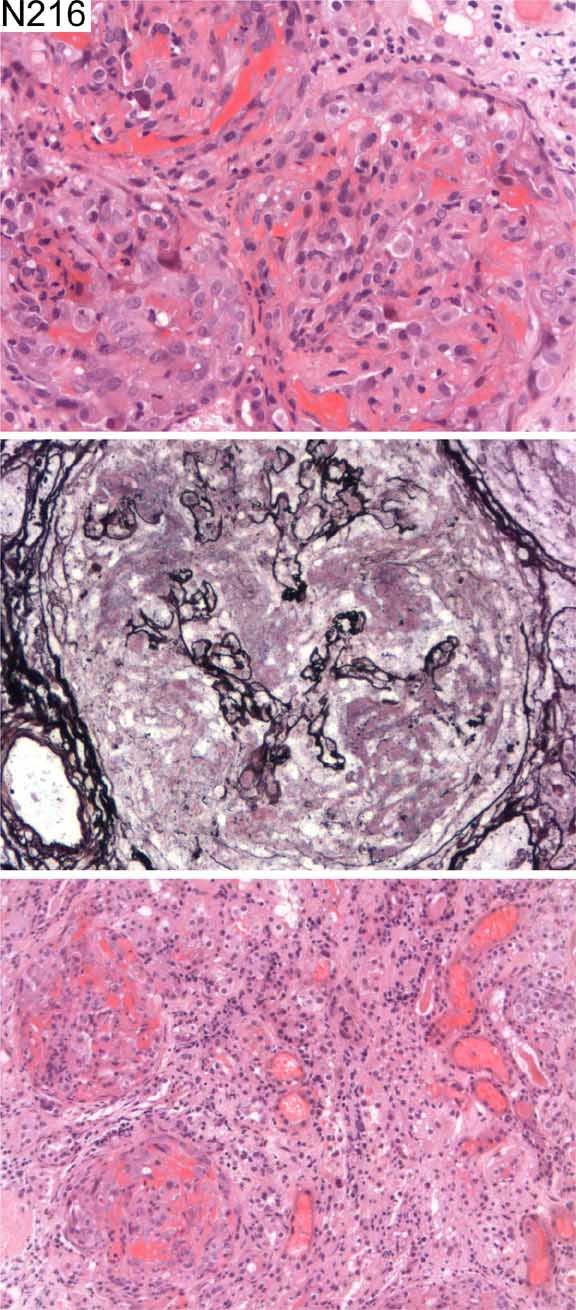
Clinical:
Male, 58 years. New acute renal failure. Urea 75, Creatinine 2187.
Oliguric. Normal sized kidneys. Antibody status not known. Two pulses of
methyl prednisolone already given. Immunofluorescence: IgA, C1q negative.
IgM +/- rather "smudged" basement membrane staining. IgG, C3 +++ linear
basement membrane positivity. C4 -/+ linear basement membrane.
Specimen:
H&E, Meth Ag
Diagnostic categories: Score:
1 Goodpasture's syndrome 9.63
2 Crescentic glomerulonephritis NOS 0.24
3 Crescentic glomerulonephritis, type I 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.63
Secondary diagnoses and comments (if any):
Lung haemorrhage?*1. Anti-GBM serology*9. ANCA?*2. EM to exclude dense
deposit disease*1. Exclude lupus*1.
Original report and further information (if any):
Acute diffuse necrotising crescentic glomerulonephritis. IF demonstrates
that this is due to Goodpasture's syndrome.
Circulation: N
Case number: 217
....
Number of responses:68 . Date of analysis: 28 DEC 03
Clinical:
Male, 47. Nephrotic syndrome. Severe ascites, albumin 34, creatinine 165.
Enlarged spleen. Normal liver bx and duodenal bx. Normal serum lipids and
LFTs. Normochromic, normocytic anaemia 9. Borderline hypopituitarism -
normal pituitary on CT. Low T4, raised prolactin and impotence. Freckles on
lips no other evidence of Peutz-Jegher syndr. Nerve conduction studies -
evidence of polyneuropathy. Nephrotic syndrome responded to steroids. IF -
diffuse mesangial A,G,M,C3.
Specimen:
H & E, PAS, EM*4
Macro:
For education and interest only
Diagnostic categories: Score:
1 Lipoprotein glomerulopathy 0.15
2 Don't know 1.18
3 Collagenofilbrotic glomerulopathy 0.15
4 Alport syndrome 0.49
5 POEMS syndrome 1.03
6 Tuberous sclerosis? 0.15
7 Immunologically mediated Gn. (incl. SLE) 1.18
8 Metabolic/storage disease NOS 3.63
9 Gaucher's disease 0.15
10 Descriptive comments only 1.91
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 8 with 3.63
Secondary diagnoses and comments (if any):
Need better EM*1. ?HIV*3. Renal vein thrombosis?*1.
Original report and further information (if any):
Case subjected to international consultation via NEPHROL. Suggestions
included Whipple's disease (excluded) and lipoprotein glomerulopathy but no
conclusion. Later developed Raynaud's. Skin bx - ?scleroderma. Developed
weakness, leg ulcers, cardiomegaly. Condition deteriorated, died, no
autopsy. Never had paraprotein. Conclusion: 'POEMS without the P'!
Links to cases in this document:
Top
N 212
N 213
N 214
N 215
N 216
N 217
Last updated: 28 DEC 03
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk