National Renal Pathology E.Q.A. Scheme
Circulation M
This document gives information on individual cases in
circulation M of this scheme. It contains no personal details
of participants.
Cases included:
M 206
M 207
M 208
M 209
M 210
M 211
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: M
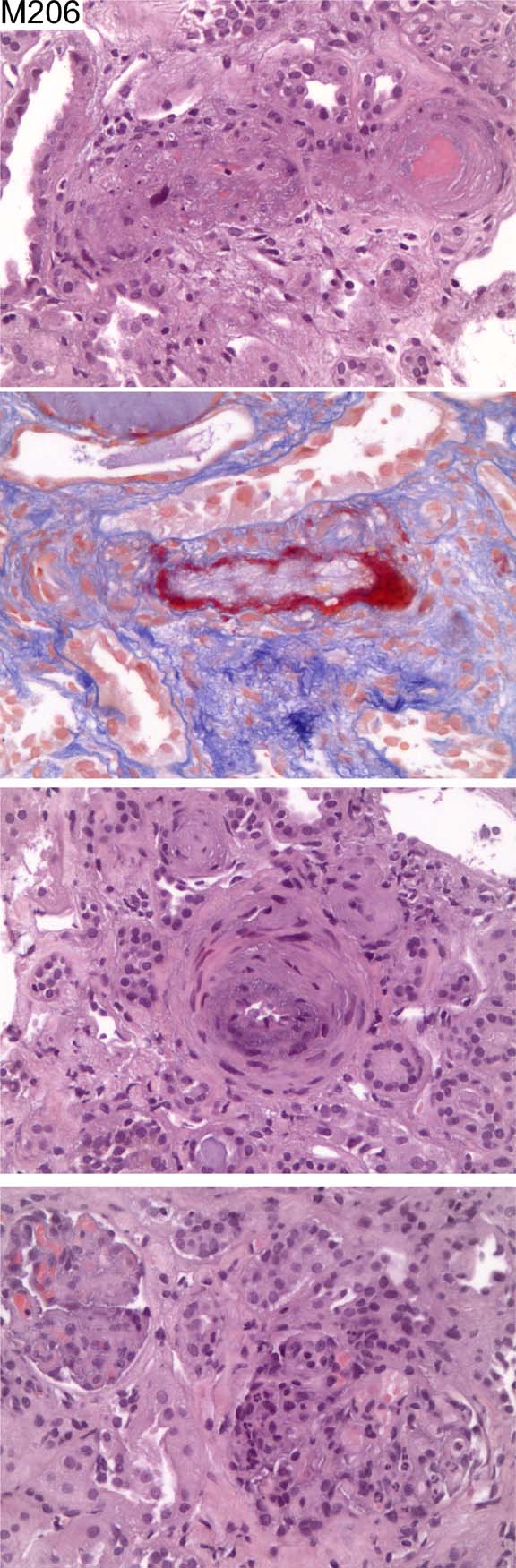
Case number: 206
....
Number of responses:81 . Date of analysis: 28 DEC 03
Clinical:
Female, 43 yrs old with abdominal pain; elevated serum creatinine level (4.
25mg/dl); microhaematuria; proteinuria of 0.9mg/dl; oliguria (500ml/24h);
anaemia; history of continuous malignant hypertension.
Specimen:
H & E, SFOG (Trichrome)
Diagnostic categories: Score:
1 Malignant hypertension 6.05
2 Malignant hypertension ? underlying Gn 0.25
3 Thrombotic microangiopathy c/w malignant HT 2.27
4 Arteriosclerosis 0.06
5 Ischaemia 0.06
6 Thrombotic microangiopathy 0.81
7 Systemic sclerosis 0.12
8 Collagenofibrotic glomerulopathy 0.12
9 Membranoproliferative Gn and hypertension 0.12
10 Refused to offer diagnosis - section quality poor 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.05
Secondary diagnoses and comments (if any):
Silver*3. Immuno. *7. EM*5. PAS*1. MSB*1. EVG*1. Exclude other causes of
microangiopathy*10. Exclude scleroderma*5. More clinical info.*1.
Autoantibodies?*1. ANCA?*1. Technical quality too poor for EQA*7.
Unsuitable for EQA*2.
Original report and further information (if any):
Circulation: M
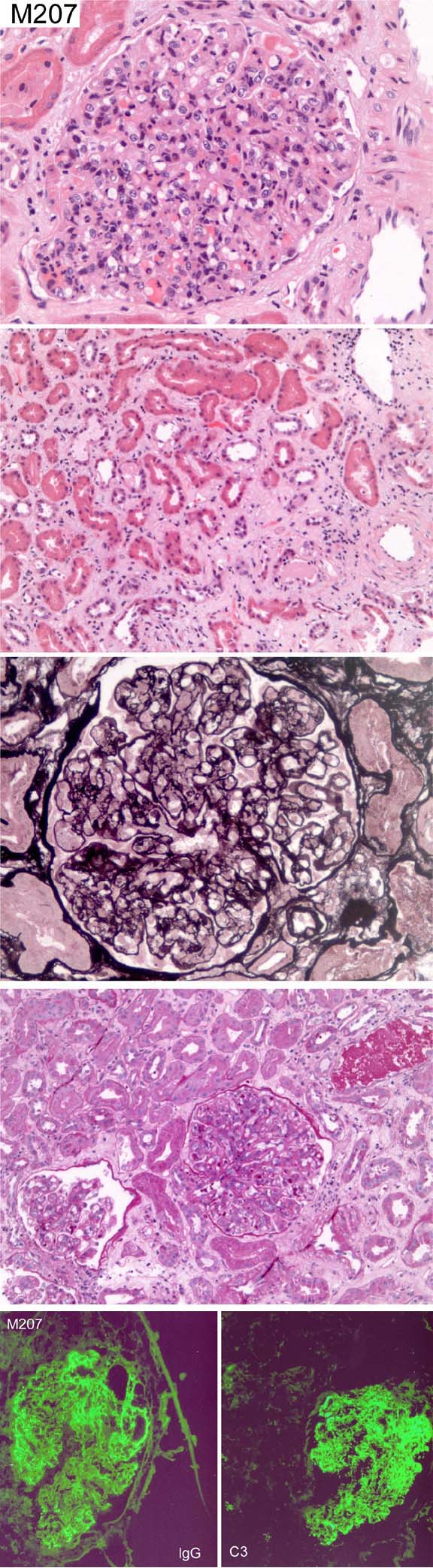
Case number: 207
....
Number of responses:81 . Date of analysis: 28 DEC 03
Clinical:
Male, 54 yrs old. Five days cough and sputum followed by gross oedema.
Creatinine 152. ASO titre equivocal. EM not yet available.
Specimen:
H & E, PAS, PASM, photos of C3, IgG
Diagnostic categories: Score:
1 Diffuse endocapillary proliferative Gn 8.53
2 Mesangiocapillary pattern Gn 0.98
3 Cryoglobulinaemia 0.12
4 Proliferative Gn 0.12
5 Mesangiocapillary Gn - post-infectious 0.12
6 Membranous glomerulonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.53
Secondary diagnoses and comments (if any):
EM*21. Other immuno results?*4. Exclude causes of mesangiocapillary
pattern*2. Exclude lupus*2. Repeat ASOT*4. Throat swab*1. Viral titres*
1. C3*1. ATN too*2. History of sepsis?*1. Inadequate for EQA*2.
Original report and further information (if any):
EM subsequently showed subepithelial 'humps' and smaller subendothelial
deposits. Creatinine went up to 434 then fell to 172. CRP always low; ANCA
and anti-GBM always negative.
Circulation: M
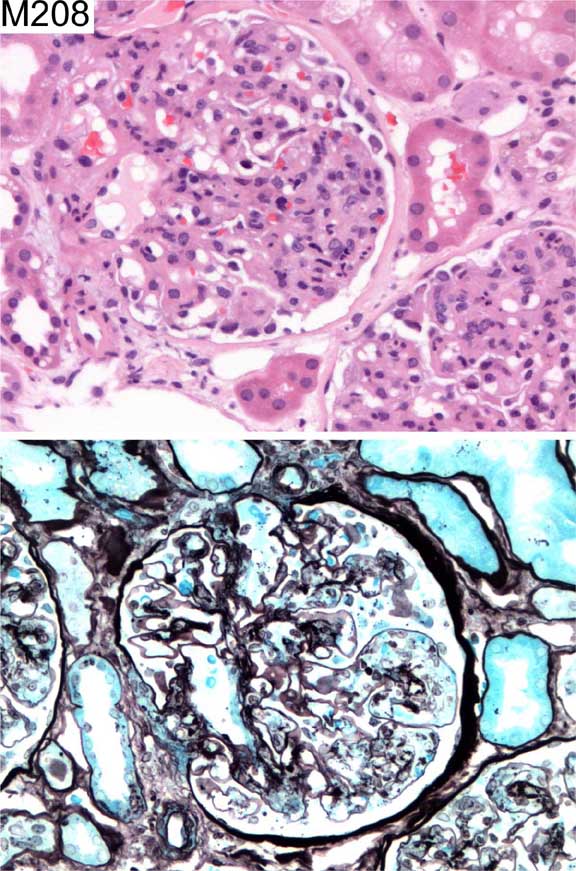
Case number: 208
....
Number of responses:81 . Date of analysis: 28 DEC 03
Clinical:
Female, 60 yrs old. Polyneuropathy, polyarthropathy, vasculitic rash
affecting lower limbs, protein+, blood+, ANCA negative, raised IgA,
creatinine 140. IF - mesangial IgA and C3.
Specimen:
H & E, Meth Ag
Diagnostic categories: Score:
1 Henoch Schonlein purpura 5.43
2 IgA nephropathy 1.48
3 HSP/IgA nephropathy 2.84
4 Membranoproliferative Gn 0.12
5 Proliferative glomerulonephritis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.43
Secondary diagnoses and comments (if any):
ASOT*1. EM*6. Secondary to autoimmune arthropathy?*1.Rather old for HSP?*2.
Exclude lupus*4. Exclude cryoglobulinaemia*1. Undetected IgA ANCA?*1.
Original report and further information (if any):
Morphologically IgA nephropathy. After clinical discussion: Henoch-
Schonlein purpura.
Circulation: M
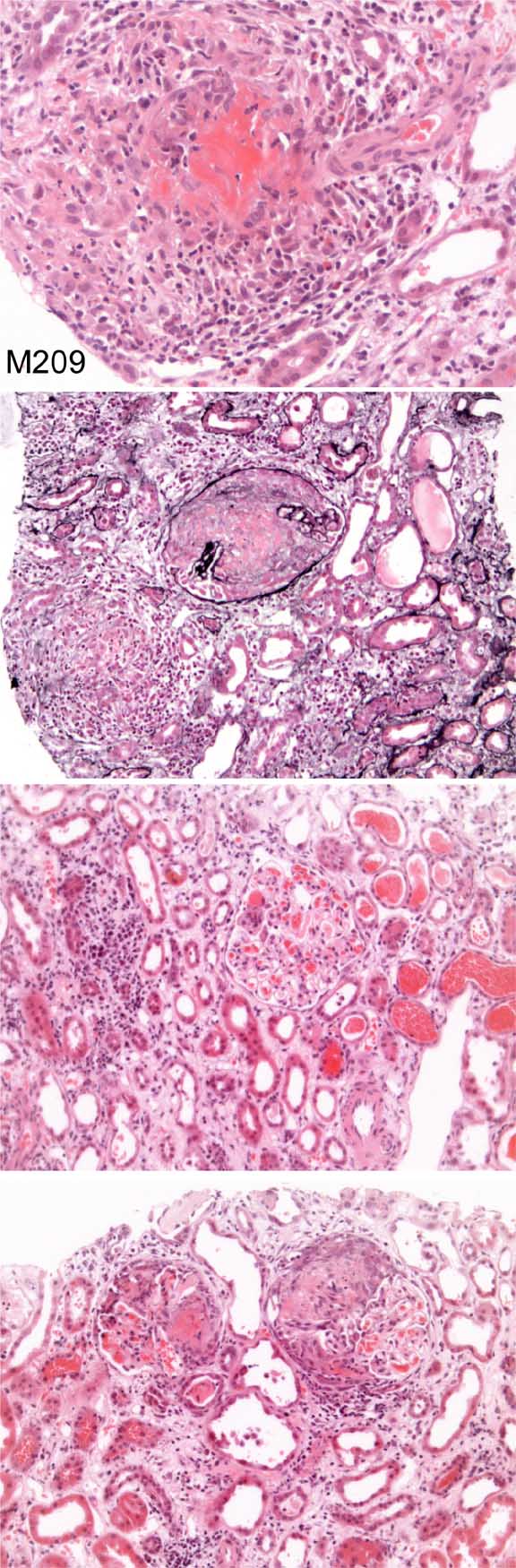
Case number: 209
....
Number of responses:81 . Date of analysis: 28 DEC 03
Clinical:
Male, 52 yrs old with multisystem disease with renal involvement, sinusitis,
pyrexia, blood+, protein+ ?vasculitis. Immunostaining negative.
Specimen:
H & E, Silver
Diagnostic categories: Score:
1 Pauci-immune necrotising Gn 7.53
2 Microscopic polyangiitis 0.37
3 Wegener's granulomatosis 1.98
4 Vasculitis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.53
Secondary diagnoses and comments (if any):
ANCA*30. EM*1. Lupus serology?*1. Churg Strauss?*1. Blood eosinophilia?*
2. CXR*3. Secondary ATN*2. ANA*1. Anti-GBM*1.
Original report and further information (if any):
Circulation: M
Case number: 210
....
Number of responses:81 . Date of analysis: 28 DEC 03
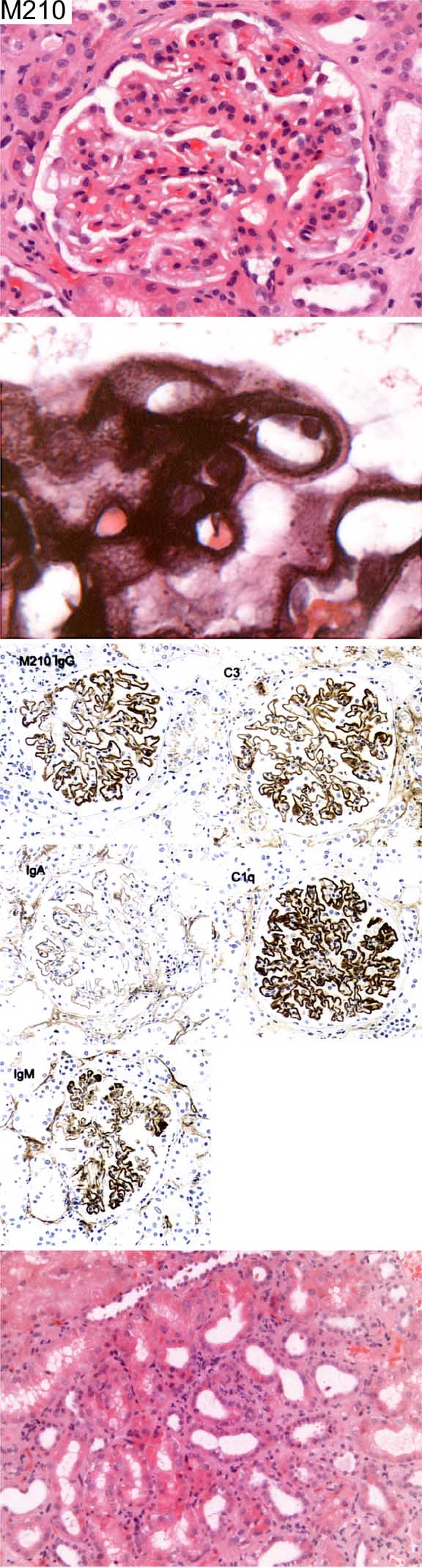
Clinical:
Male, 54 yrs old. Nephrotic syndrome, no obvious cause.
Specimen:
H & E; Silver; Photos of C3c, C1q, IgM, IgA, IgG
Diagnostic categories: Score:
1 Membranous glomerulonephritis 9.67
2 Membranous Gn due to SLE 0.33
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.67
Secondary diagnoses and comments (if any):
Exclude SLE*39. Exclude hepatitis B*1. Drug history?*2. Malignancy?*2. EM*
6. Exclude mesangiocapillary Gn with EM*1. Glomerular tip lesion present*
1. H&E too pale*5.
Original report and further information (if any):
Membranous nephropathy. ANA negative.
Circulation: M
Case number: 211
....
Number of responses:69 . Date of analysis: 28 DEC 03
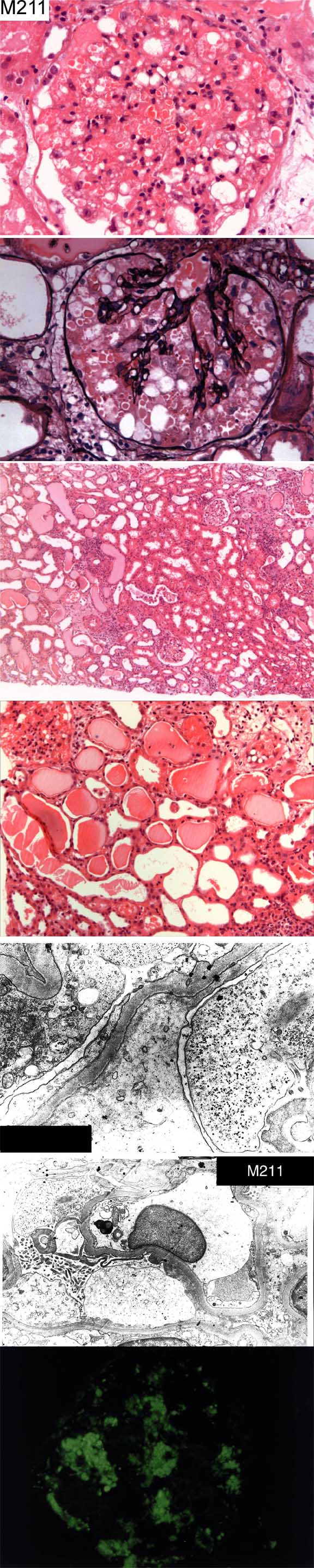
Clinical:
Male, 45 y.o. Malaria following trip to Nigeria (low parasitaemia).
Presented with creatinine 1200 with no previous renal problems. Urine 4+
blood, 4+ protein. HIV serology performed following biopsy - negative.
Hyalinotic resorption droplets within podocytes are positive with IgG, IgA
and C3 but these antibodies are otherwise negative. There is weak focal
positivity for IgM (+/-) in glomerular capillary walls.
Specimen:
H & E Photos - Meth Ag, C3, IF, EM*2
Macro:
For education and interest
Diagnostic categories: Score:
1 No idea. 1.16
2 Collapsing glomerulopathy 3.62
3 Malarial nephropathy 2.83
4 HIV nephropathy (despite serology) 1.09
5 Focal segmental glomerulosclerosis 0.29
6 ATN 0.65
7 Drug reaction? 0.07
8 Minimal change nephropathy 0.14
9 Acute interstitial nephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 3.62
Secondary diagnoses and comments (if any):
Consider HIV*1. Repeat HIV test*7. ATN too*2. Hep.B?*1. Changes in
tubules ??CMV*1. Sickle cell disease?*1. Drug reaction?*1
Original report and further information (if any):
Function recovered - creatinine 200 2 yrs later. Still has 2g poteinuria.
Looked like a collapsing glomerulopathy but isn't behaving like one.
Believed to be all secondary to falciparum malaria.
Links to cases in this document:
Top
M 206
M 207
M 208
M 209
M 210
M 211
Last updated: 28 DEC 03
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk