National Renal Pathology E.Q.A. Scheme
Circulation K
This document gives information on individual cases in
circulation K of this scheme. It contains no personal details
of participants.
Cases included:
K 194
K 195
K 196
K 197
K 198
K 199
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: K
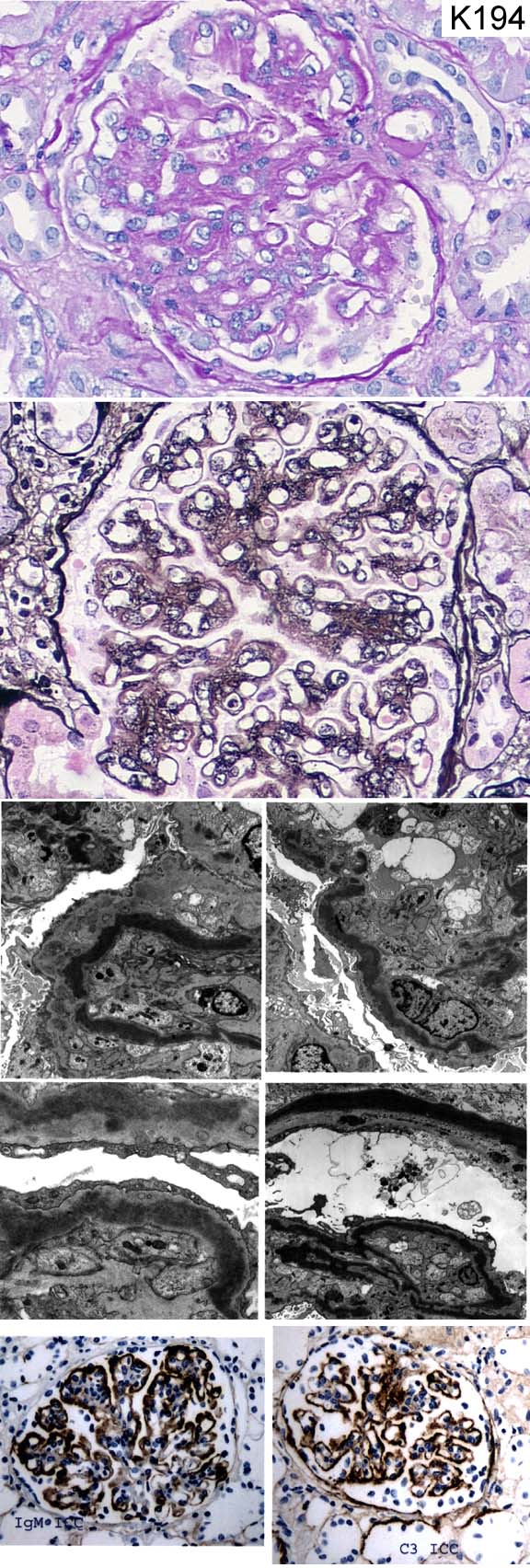
Case number: 194
....
Number of responses:81 . Date of analysis: 27 APR 03
Clinical:
12 year old girl, recent onset of nephrotic syndrome. Steroid resistant.
ANA negative.
Specimen:
PAS, Meth Ag, Photos of EM*4, IgM, C3
Diagnostic categories: Score:
1 Dense deposit disease (MCGn type II) 9.63
2 Membranoproliferative Gn type I 0.12
3 IgM nephropathy 0.12
4 Mesangiocapillary Gn (type not mentioned) 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.63
Secondary diagnoses and comments (if any):
Serum C3 level?*4. C3Nef?*3. Family history?*1. Lipodystrophy?*4. Exclude
hepatitis B, C*2. Exclude cryoglobulins*1.
Original report and further information (if any):
Circulation: K
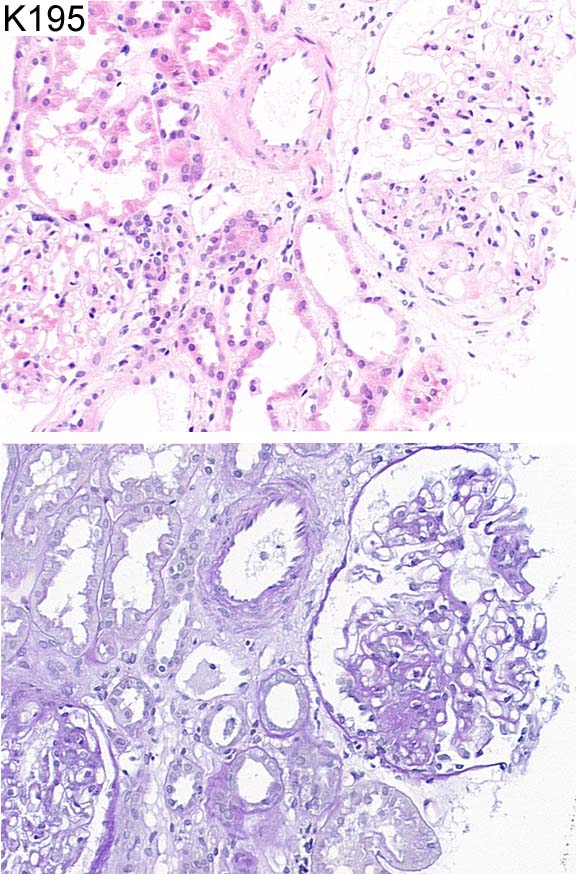
Case number: 195
....
Number of responses:81 . Date of analysis: 27 APR 03
Clinical:
37 year old man with focal segmental glomerulosclerosis. Presented with
nephrotic syndrome without any relevant medical history. Immunofluorescence
was negative> Electron microscopy showed swelling of the visceral
epithelial cells and global effacement of the foot processes. No deposits
seen.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Focal segmental glomerulosclerosis 9.58
2 Minimal change nephropathy 0.30
3 Glomerular tip lesion 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.58
Secondary diagnoses and comments (if any):
ATN too*5. 'Tip' lesion too*6. HIV status?*5. Exclude amyloid*2. Why's the
diagnosis in the clinical info?*6. Exclude CMV*1. Silver*2. Deeper
sections*1. Pale H&E*4.
Original report and further information (if any):
Focal segmental glomerulosclerosis. No further information; followed up
elsewhere.
Circulation: K
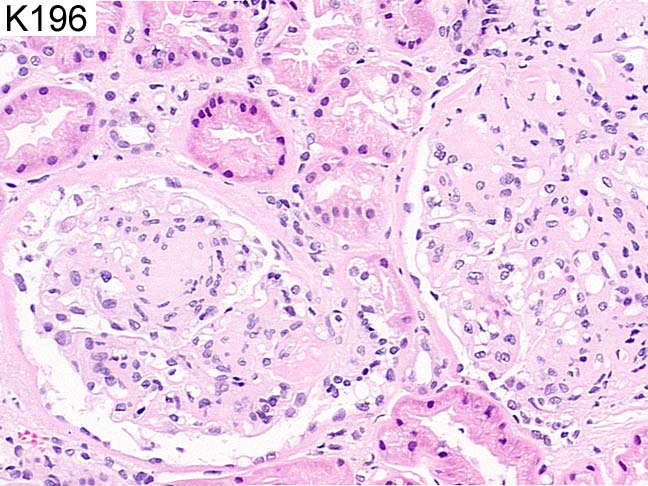
Case number: 196
....
Number of responses:81 . Date of analysis: 27 APR 03
Clinical:
Diabetic for 20 years, Creatinine 169, hypertensive, haematuria for 5 years
macroscopically, raised proteinuria with time. Now nephrotic. ?DM
nephropathy, ?other GN eg membranous. Immunofluorescence all negative.
Silver stain shows normal capillary basement membranes.
Specimen:
H&E
Diagnostic categories: Score:
1 Diabetic nephropathy 9.15
2 Amyloid 0.21
3 Nodular glomerulosclerosis 0.12
4 Light chain disease 0.07
5 Immunotactoid Gn 0.01
6 Cryoglobulinaemia 0.05
7 Focal segmental glomerulosclerosis 0.12
8 Mesangial proliferative glomerulonephritis 0.01
10 Refusal to interpret pale H&E 0.25
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.15
Secondary diagnoses and comments (if any):
EM needed*18. Basement membrane measiurement?*1. Congo red *18. Immuno
needed*5. No linear IgG unusual in diabetes*2. Immunoelectrophoresis *1.
Kappa & lambda*5. Silver*7. PAS*5. EVG*1. Also interstitial nephritis*
10. Slide too pale*18. Inadequate for EQA*10.
Original report and further information (if any):
Advanced diabetic nephropathy. (E.M. subsequently consistent with that
diagnosis)
Circulation: K
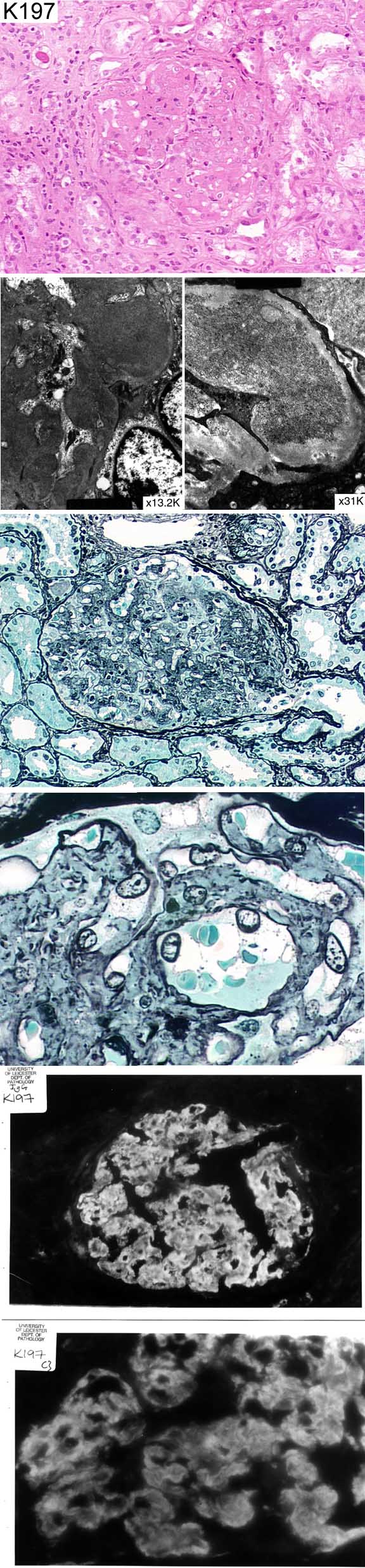
Case number: 197
....
Number of responses:81 . Date of analysis: 27 APR 03
Clinical:
Female 49. Nephrotic syndrome with acute renal failure. Hypoproteinaemia,
proteinuria++, haematuria+++. Admitted with ?malignant hypertension.
Specimen:
H&E, Methenamine Silver, IgG, C3, EM*3
Diagnostic categories: Score:
1 Fibrillary glomerulopathy 5.15
2 Immunotactoid glomerulopathy 1.78
3 Amyloid 2.61
4 Cryoglobulinaemia 0.43
5 Mesangiocapillary Gn 0.04
10 1 and 2 will need to be merged - PF. 0.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.15
Secondary diagnoses and comments (if any):
Need scale on EM for fibril size*22. Higher mag. EM of fibrils*7. Lupus
serology*4. Exclude diabetes*1. Rest of immuno.*2. Congo Red*45. Serum
electrophoresis*6. Kappa & lambda immuno*8. Cryoglobulins?*8. Autoantibody
screen*1. Hypertensive vessels*4. Poor H&E*7. Unsuitable for EQA*4.
Original report and further information (if any):
Fibrillary glomerulonephritis. Given symptomatic treatment only. Remains
nephrotic; creatinine has since risen from 250 to 400.
Circulation: K
Case number: 198
....
Number of responses:81 . Date of analysis: 27 APR 03
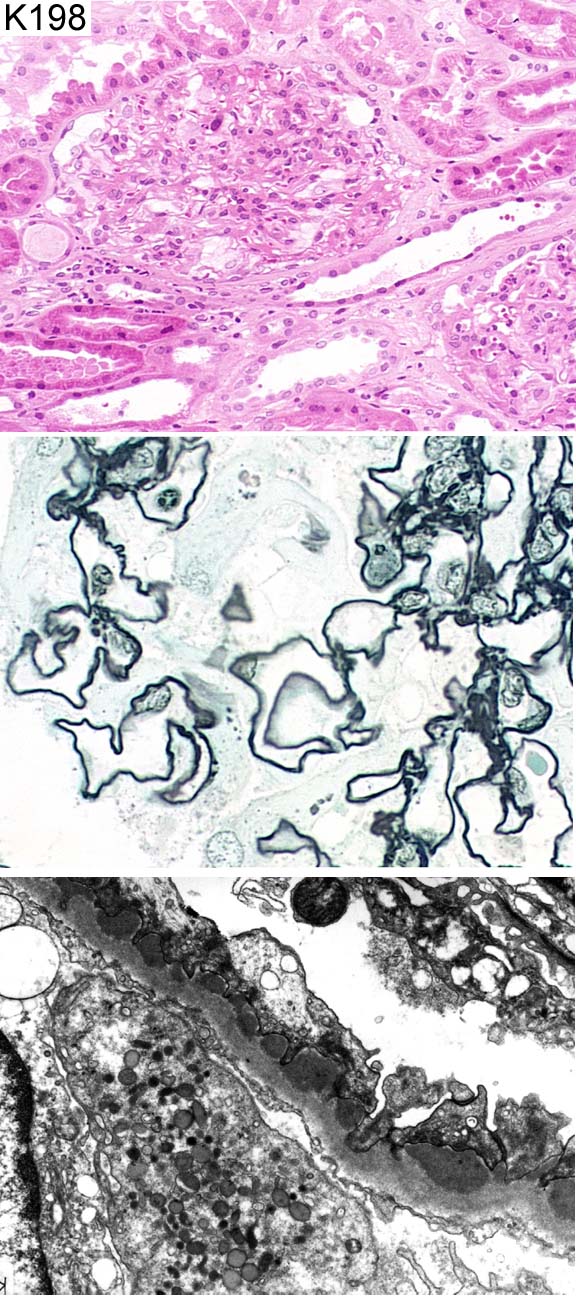
Clinical:
66 year old male with past history of asthma and elevated eosinophils in the
past as well as hypertension. The patient was admitted with ++++proteinuria
and ++haematuria. The only abnormal clinical parameter at the time of the
biopsy was CRP of 17. The immunofluorescence of the case showed linear IgG
and C3 staining, glomerular basement membrane antibodies were negative.
Specimen:
H&E, Meth Ag, EM
Diagnostic categories: Score:
1 Membranous Gn 8.31
2 Atypical membranous ? secondary 0.49
3 Churg Strauss syndrome 0.19
4 Mesangial proliferative Gn 0.21
5 Vasculitis 0.19
6 Post-infectious glomerulonephritis 0.25
7 Churg Strauss AND membranous Gn. 0.12
8 Focal segmental glomerulonephritis 0.12
9 Membranous Gn AND granulomatous vasculitis 0.12
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.31
Secondary diagnoses and comments (if any):
Was the IF REALLY linear??*6. 'Linear' IF presumably really v. finely
granular*6. Eosinophils present *7. Exclude parasites *1. Interstitial
nephritis too*3. ?related to asthma?*1. ?Churg-Strauss*4. ?vasculitis*2.
ANCA*1. ?RVT*1. ASOT?*1. Suitable for EQA?*1.
Original report and further information (if any):
Early membranous glomerulonephritis. No explanation found for interstitial
eosinophils. Glomerular microthrombi noted; patient later developed DVT.
Subsequent decline in renal function from creatinine 101 to 220 over 1
year.
Circulation: K
Case number: 199
....
Number of responses:81 . Date of analysis: 27 APR 03
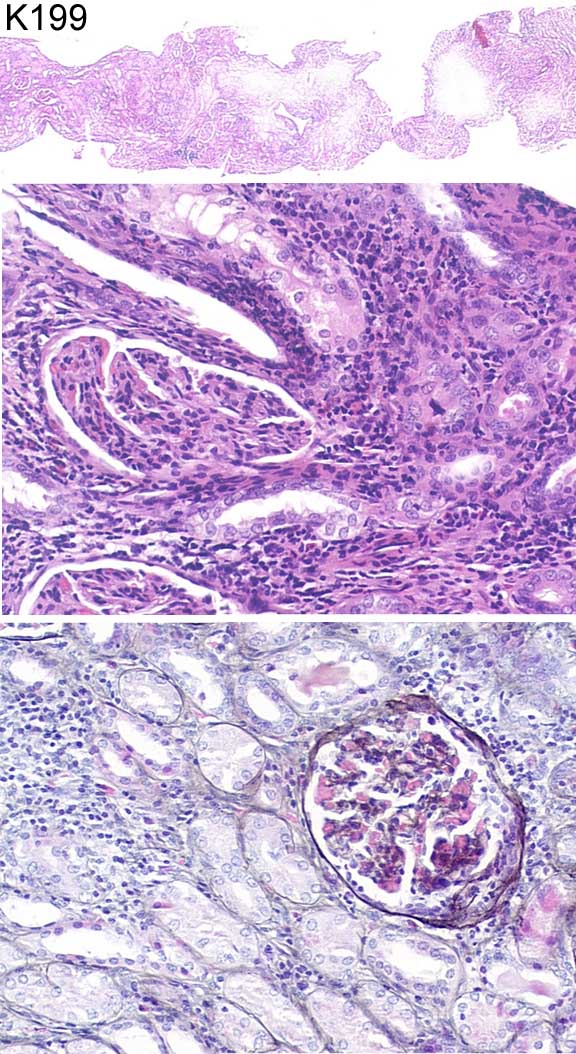
Clinical:
10 year old boy with proteinuria, haematuria, phosphaturia, glycosuria.
Probable tubulo-interstitial nephritis with uveitis. Immunohistology
negative. EM: Small segments of foot process fusion. Nil else
significant.
Specimen:
H&E, Meth Ag
Diagnostic categories: Score:
1 Acute tubulo-interstitial nephritis 1.48
2 Tubulo-interstitial nephritis NOS 2.10
3 T-I neprhitis and uveitis (= Dobrin's syndrome) 5.66
4 Fanconi syndrome 0.14
5 Cystinosis 0.12
6 Interstitial nephritis with granulomas (?sarcoid) 0.49
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 5.66
Secondary diagnoses and comments (if any):
Exclude toxoplasmosis*6. TIN probably allergic*2. Drug induced?*5.
Inherited disorder?*1. Exclude lymphoproliferative disease*1. Exclude
sarcoid*3. Exclude Behcet's*1. Exclude Sjogren's *1. Quantitation of
proteinuria*1. Poor section*10. Nephronophthisis too?*1. Mnimal change
too?*2. Alports too?*2. PAS*1. Z-N*1.
Original report and further information (if any):
Interstitial nephritis, in keeping with the syndrome of Tubulo-Interstitial
Nephritis with Uveitis.
Links to cases in this document:
Top
K 194
K 195
K 196
K 197
K 198
K 199
Last updated: 27 APR 03
Organiser:
Professor Peter Furness, PhD, FRCPath.
Clinical Sciences Laboratories
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk