National Renal Pathology E.Q.A. Scheme
Circulation J
This document gives information on individual cases in
circulation J of this scheme. It contains no personal details
of participants.
Cases included:
J 188
J 189
J 190
J 191
J 192
J 193
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: J
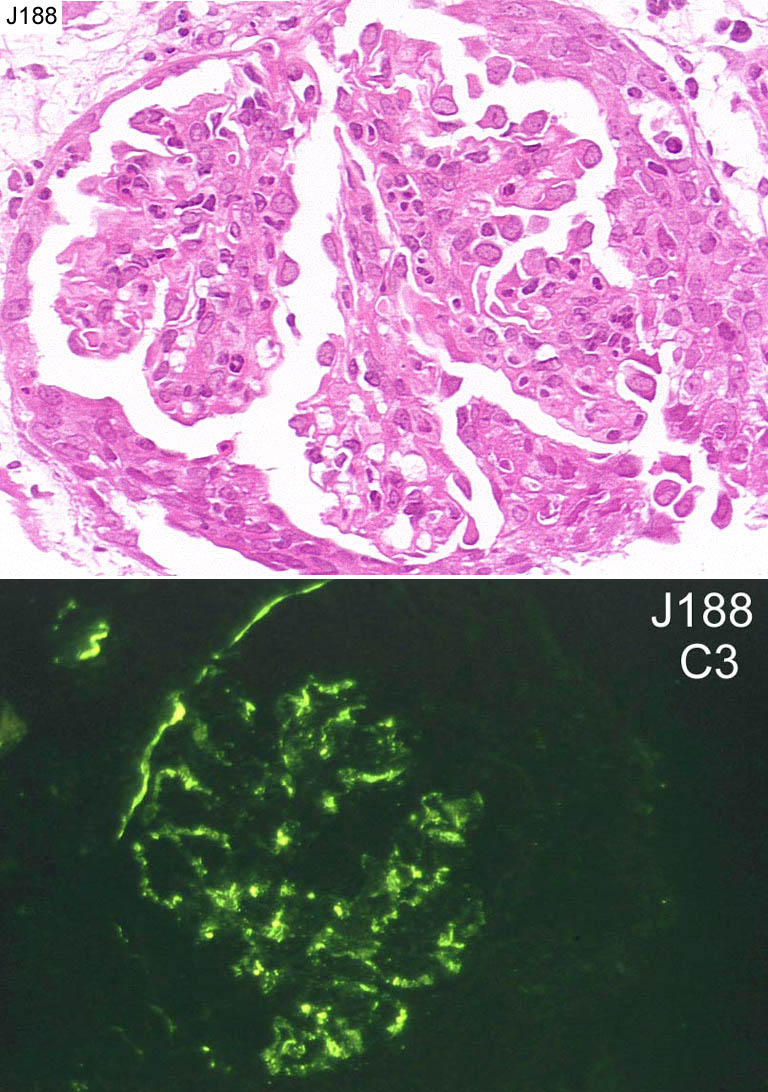
Case number: 188
....
Number of responses:72 . Date of analysis: 11 JUL 02
Clinical:
6 year Zambian boy admitted with Hb6 and acute anuric renal failure ?Gn.
Parents are HIV positive, he is HIV negative. No further serology
available. Photo of C3 is provided. Immunoglobulins and C1q were negative.
Specimen:
H&E, PAS, photo of C3
Diagnostic categories: Score:
1 Post-infectious / endocapill. prolif. Gn 4.99
2 Mesangiocapillary Gn 0.26
3 Crescentic Gn NOS 3.33
4 Mesangial prolif. Gn with crescents 0.14
5 Immune complex crecentic Gn 0.28
6 Pauci-immune crescentic Gn 0.69
7 HIV associated nephropathy 0.26
8 Diffuse proliferative Gn 0.04
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.99
Secondary diagnoses and comments (if any):
Infection related?*3. More clinical info *3. ASOT*9. ANCA*8. Anti-GBM*4.
EM*11. No PAS*5. ATN too*3. Malaria?*1. Cryoglobulins?*1. Hep C?*1. ?SLE*1.
?HIV*1.
Original report and further information (if any):
High ASOT. Re-biopsy 6 weeks later - glomerular changes resolved.
Diagnosis: Post-infective Gn.
Circulation: J
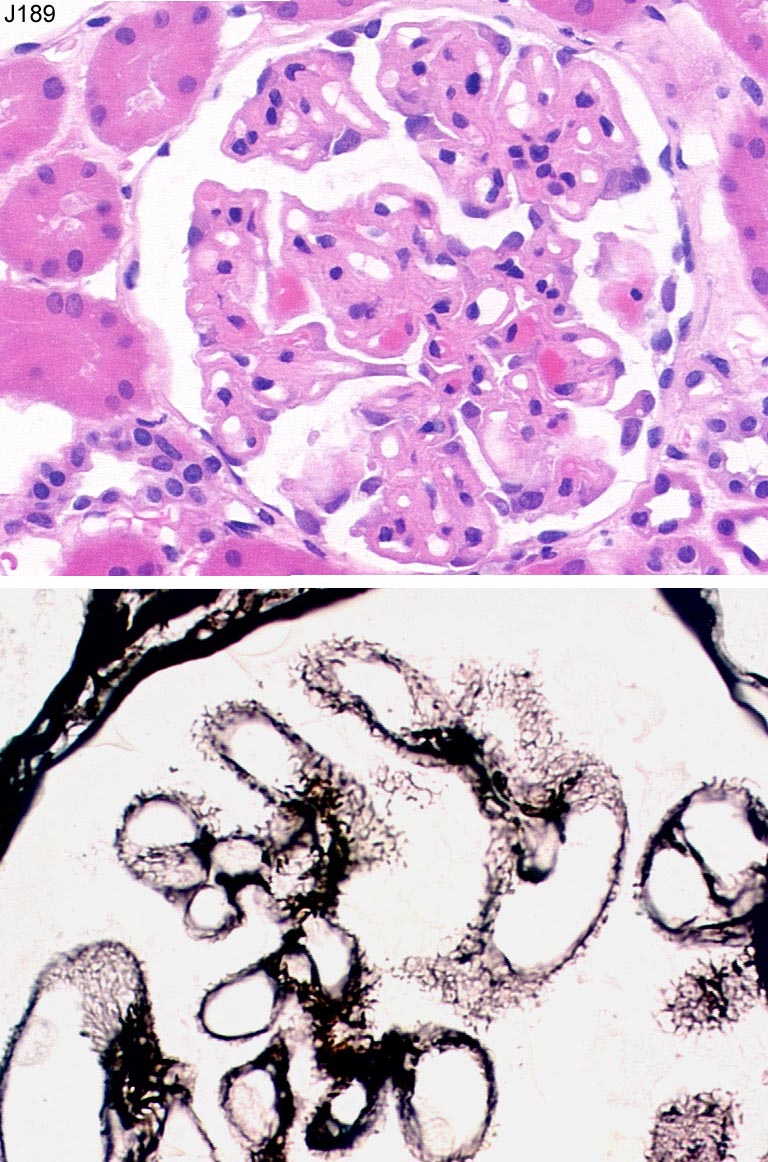
Case number: 189
....
Number of responses:72 . Date of analysis: 11 JUL 02
Clinical:
49 year old lady. 1.9g proteinuria with haematuria ? cause. Rheumatoid
arthritis treated with NSAIDs and penicillamine. Immunohistochemistry
granular positivity basement membrane IgG IgM (both strong) and weak IgA.
Complement negative.
Specimen:
H&E, silver
Diagnostic categories: Score:
1 Membranous Gn 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Penicillamine?*37. Gold?*1. Secondary membranous?*7. EM*4. ?SLE*9. Congo
red*3. Repeat IF for complement*1. Exclude diabetes*1.
Original report and further information (if any):
Circulation: J
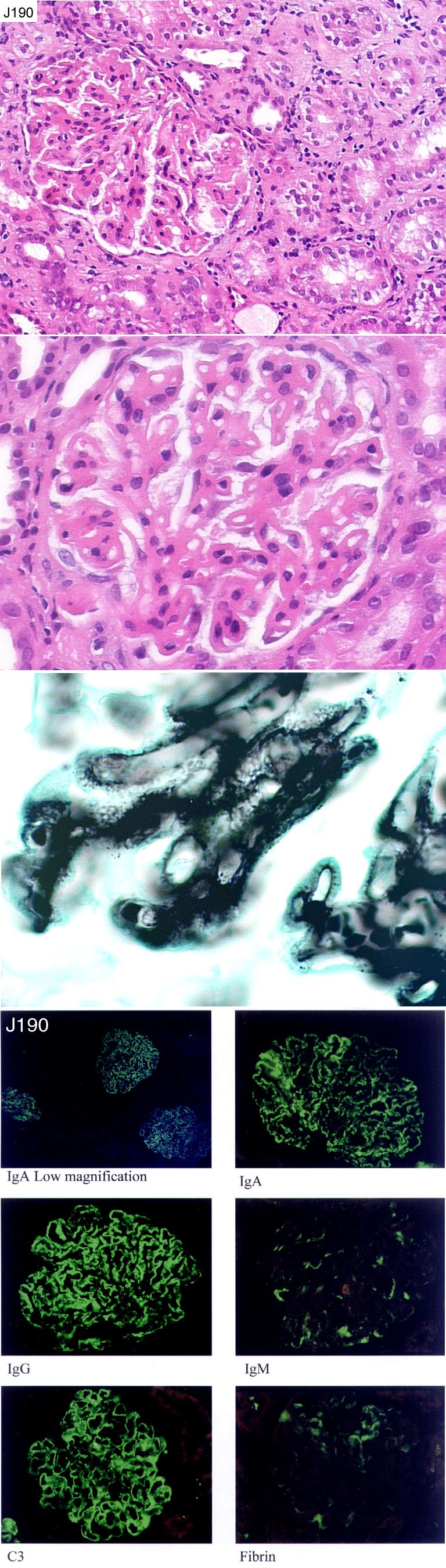
Case number: 190
....
Number of responses:71 . Date of analysis: 11 JUL 02
Clinical:
Male, 21 years old, proteinuria (4g/24h) and hypoalbuminaemia
Specimen:
H&E, PAS, silver, IF photos *6.
Diagnostic categories: Score:
1 Membranous Gn 6.69
2 Membranous Gn ?lupus 1.13
3 IgA nephropathy 0.28
4 SLE 0.70
5 Fibrillary glomerulonephritis 0.07
6 Mesangiocapillary Gn 0.99
7 Proliferative glomerulonephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.69
Secondary diagnoses and comments (if any):
EM*12. ?SLE serology*34. dsDNA*1. C1q*5. Congo red*1. Viruses?*1. Hep B?*3.
Drugs?*1. Malaria?*1. Granuloma present ? sarcoid*1. Urine culture*1.
Original report and further information (if any):
Membranous glomerulonephritis.
Circulation: J
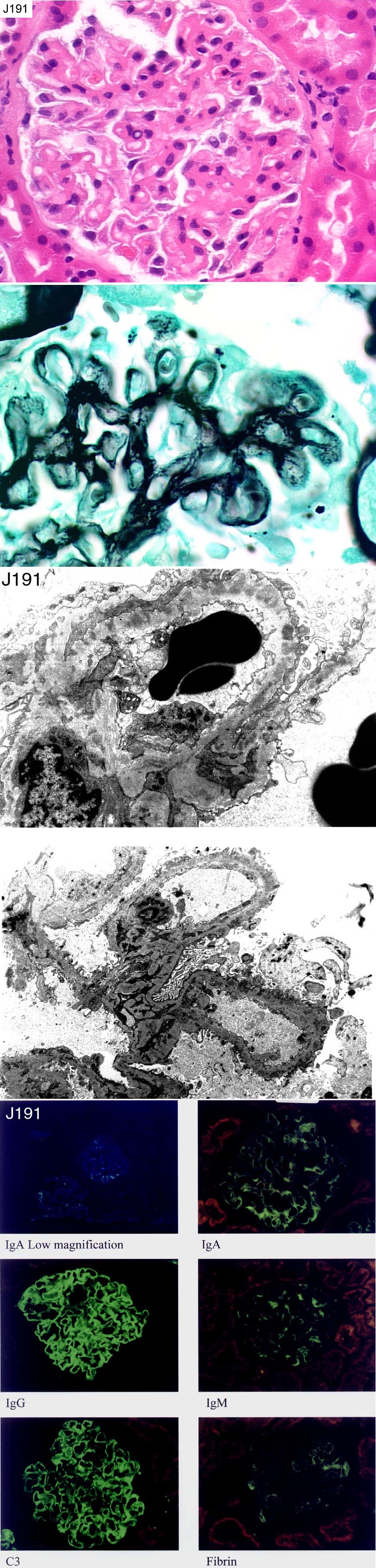
Case number: 191
....
Number of responses:71 . Date of analysis: 11 JUL 02
Clinical:
67y.o. lady with proteinuria and hypoalbuminaemia. History of tuberculosis;
was on anti-tuberculous therapy.
Specimen:
H&E, PAS, silver, IF photo*6, EM*2.
Diagnostic categories: Score:
1 Membranous Gn 9.51
2 Mesangiocapillary Gn 0.32
3 Lupus nephritis 0.17
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.51
Secondary diagnoses and comments (if any):
?SLE*11. Secondary?*4. Drugs?*11. ?Malignancy*1. EM*1. Hypertensive
changes too*1. C1q*2. C4*1, ?tubuloreticulars on EM?*1. TB therapy
coincidental?*2.
Original report and further information (if any):
Membranous glomerulonephritis.
Circulation: J
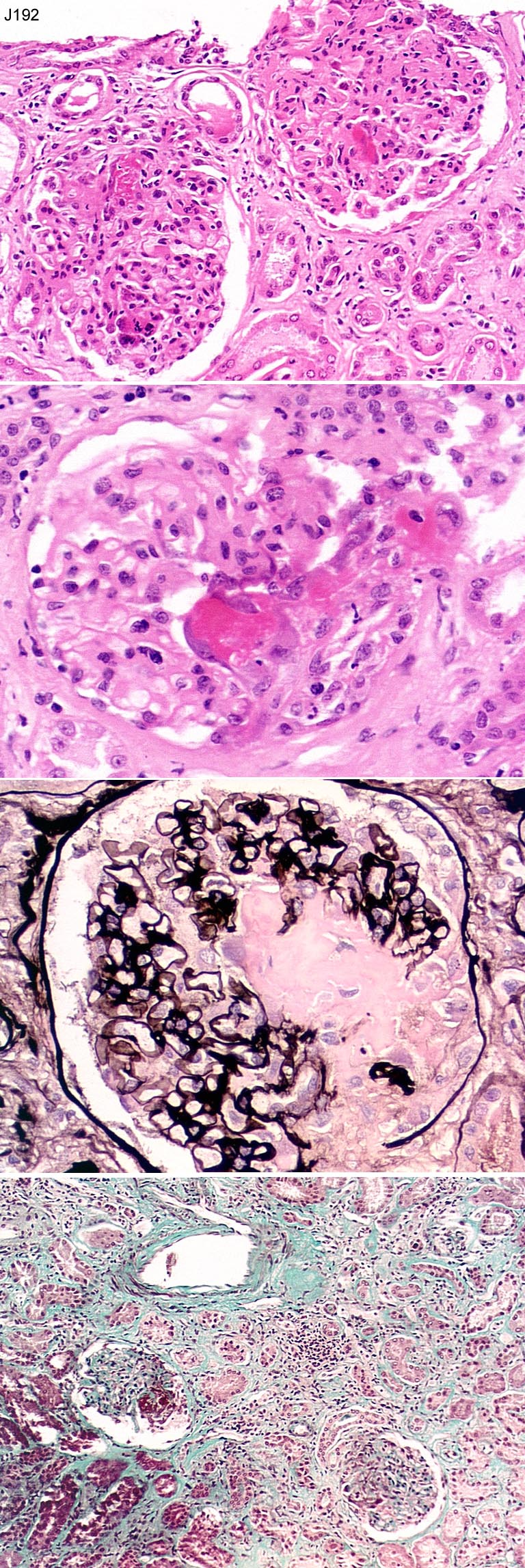
Case number: 192
....
Number of responses:70 . Date of analysis: 11 JUL 02
Clinical:
64 y.o. lady. Severe nephrotic syndrome with deteriorating renal function.
History of congenital heart disease, seems to have RHF. Raised CRP.
Serology negative. NB only on core, frozen for IF before paraffin
processing. IF: C3 and IgM in mesangium and capillary walls, fibrin in a few
glomerular segments. Arterioles focally positive for C3
Specimen:
H&E, masson trichrome, silver
Diagnostic categories: Score:
1 Necrotising Gn c/w vasculitis 1.71
2 Focal / segmental glomerulonephritis 0.43
3 Necrotising Gn, ?due to infective endocarditis 5.47
4 Necrotosing Gn, differential given 0.60
5 Necrotising Gn NOS 0.71
6 Acute postinfective Gn 0.29
7 Focal necrotising Gn, 'embolic' (endocarditis?) 0.43
8 Cryoglobulinaemia 0.07
9 Thrombotic microangiopathy ?due to endocarditis 0.14
10 No response 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 5.47
Secondary diagnoses and comments (if any):
Exclude cryoglobulins*3. Exclude infective endocarditis / do
echocardiogram*10. Why nephrotic?*1. Does 'negative serology' include
ANCA?*3. ANCA*6. Exclude SLE*3. Anti-GBM*2. EM*3.
Original report and further information (if any):
1 week after biopsy, blood cultures positive S. aureus, vegetations on
pulmonary valve. Dialysis dependent. Treated with antibiotics; renal
function improved to creatinine 127. Severe RHF. Died of inoperable heart
disease (transposition and pulmonary hypertension) 10 montha after
biopsy.
Circulation: J
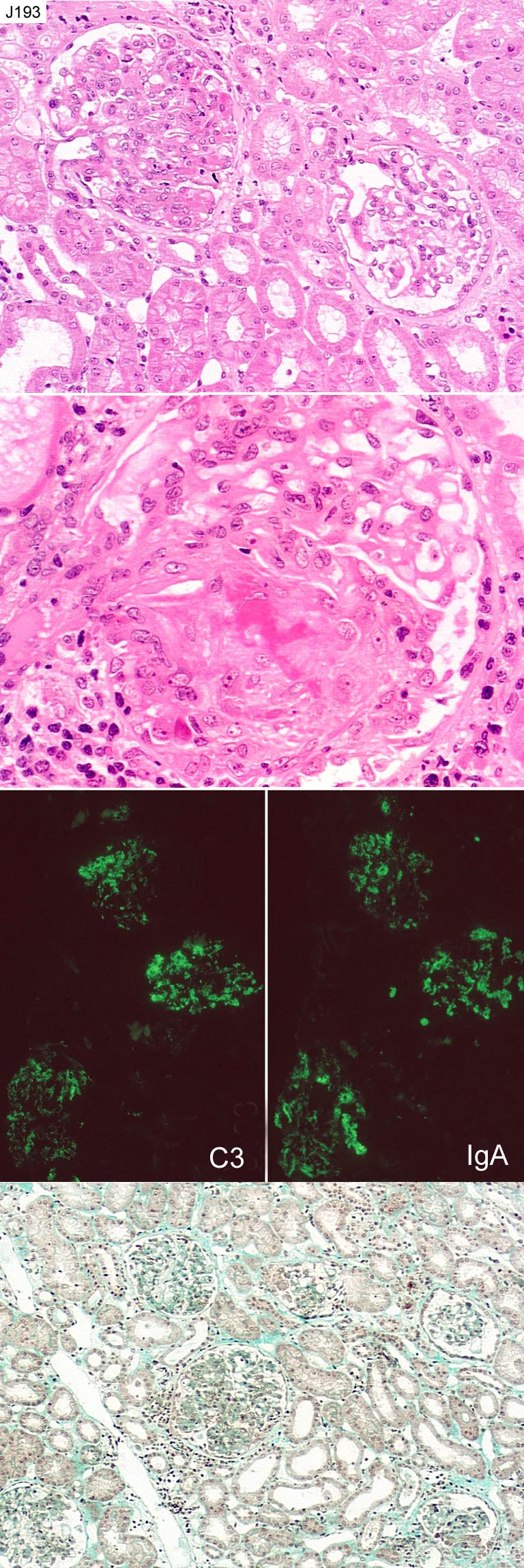
Case number: 193
....
Number of responses:70 . Date of analysis: 11 JUL 02
Clinical:
21 year old man with 3 week history of rash. BP normal. Creatinine 228. Has
haematuria and proteinuria - ? chronic and acute changes?
Specimen:
H&E, Masson trichrome, silver, IF images *2.
Diagnostic categories: Score:
1 Henoch Schonlein purpura/IgAN, acute 4.00
2 HSP/ IgAN, acute/chronic not mentioned 4.86
3 HSP / IgAN, chronic 0.14
4 IgA nephropathy (HSP not mentioned) 0.86
10 No response 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 4.86
Secondary diagnoses and comments (if any):
EM*2. Rest of immuno panel?*1. dsDNA*1.
Original report and further information (if any):
Acute Henoch Schonlein purpura. A skin biopsy showed IgA, C3 and fibrin
in dermal blood vessels.
Links to cases in this document:
Top
J 188
J 189
J 190
J 191
J 192
J 193
Last updated: 11 JUL 02
Organiser:
Professor Peter Furness, PhD, FRCPath.
Clinical Sciences Laboratories
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk