National Renal Pathology E.Q.A. Scheme
Circulation H
This document gives information on individual cases in
circulation H of this scheme. It contains no personal details
of participants.
Cases included:
H 182
H 183
H 184
H 185
H 186
H 187
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: H
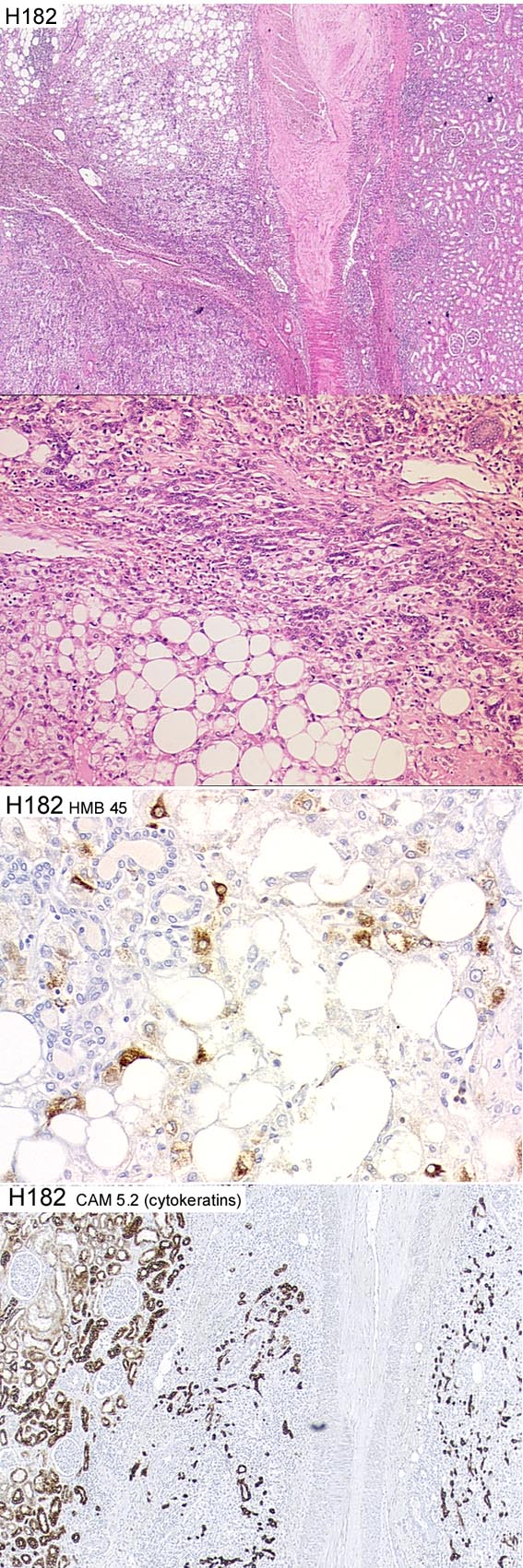
Case number: 182
....
Number of responses:74 . Date of analysis: 11 JUL 02
Clinical:
Female, 30 years old. Acute renal bleed, Hb down to 6. CAT- large
haematoma lower pole L kidney. Tumour circulation on angiogram.
Specimen:
Nephrectomy for tumour
Macro:
Large haematoma round pale tumour 5cm in diamter, lower pole. Uninvolved
kidney grossly normal. Supplied H&E of tumour edge; images of CAM5.2 and
HMB45.
Diagnostic categories: Score:
1 Angiomyolipoma 9.93
2 Clear cell sarcoma 0.07
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.93
Secondary diagnoses and comments (if any):
History to exclude malignancy*1. Tuberose sclerosis?*8. Entrapped tubules
noted*10. Angiomyo and clear cell sarcoma both HMB45 positive*1. Photos
not received*2.
Original report and further information (if any):
Benign angiolipoma with entrapment of renal tubules at edges.
Circulation: H
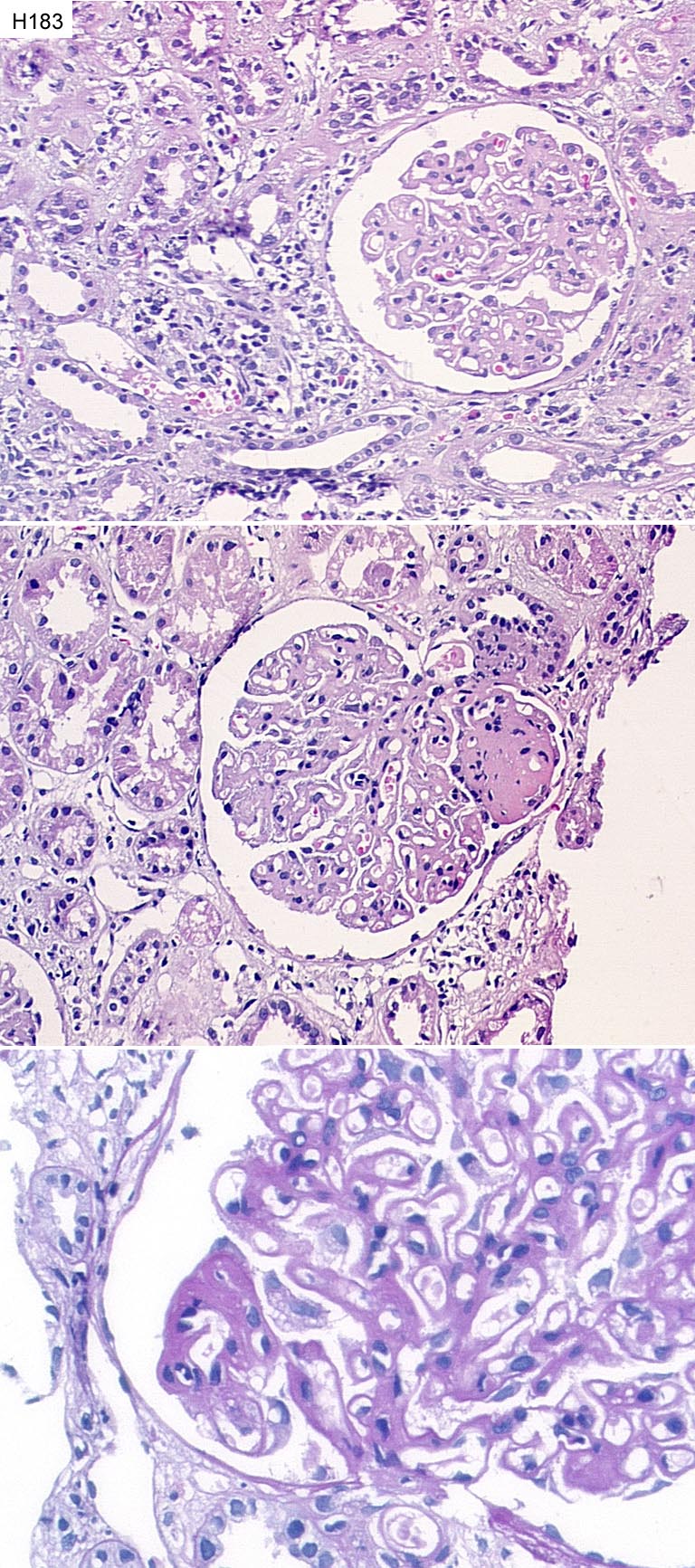
Case number: 183
....
Number of responses:75 . Date of analysis: 11 JUL 02
Clinical:
Male, 19y.o. Hypertension (160/100) and proteinuria 7g. found one year ago.
Treated with ACE inhibitor. BP dropped to 140/90, proteinuria fell to 3.5g.
Normal creatinine. Ultrasound of kidneys normal. IF: Granular capillary
basement membrane IgG++ with C3+, some IgA in tubules. No EM.
Specimen:
H&E, PAS
Macro:
(Case from outside UK: This may or may not be relevant)
Diagnostic categories: Score:
1 Membranous nephropathy 9.69
2 Mesangiocapillary Gn 0.13
3 Diabetic 'membranous Gn' 0.17
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.69
Secondary diagnoses and comments (if any):
Segmental lesions present*13. Silver*19. EM*14. EVG*1. Secondary
membranous?*10. Lupus serology?*8. Diabetes too?*2. Interstitial nephritis
too*2. Inadequate mateial for EQA*4. Congo red*3. ?Sickle cell disease?*
1.
Original report and further information (if any):
Diffuse membranous nephropathy with segmental sclerotic changes, plus mild
interstitial nephritis with eosinophils, possibly drug induced. 1 week
later developed ARF with eosinophils in urine. Given steroids; renal
function improved.
Circulation: H
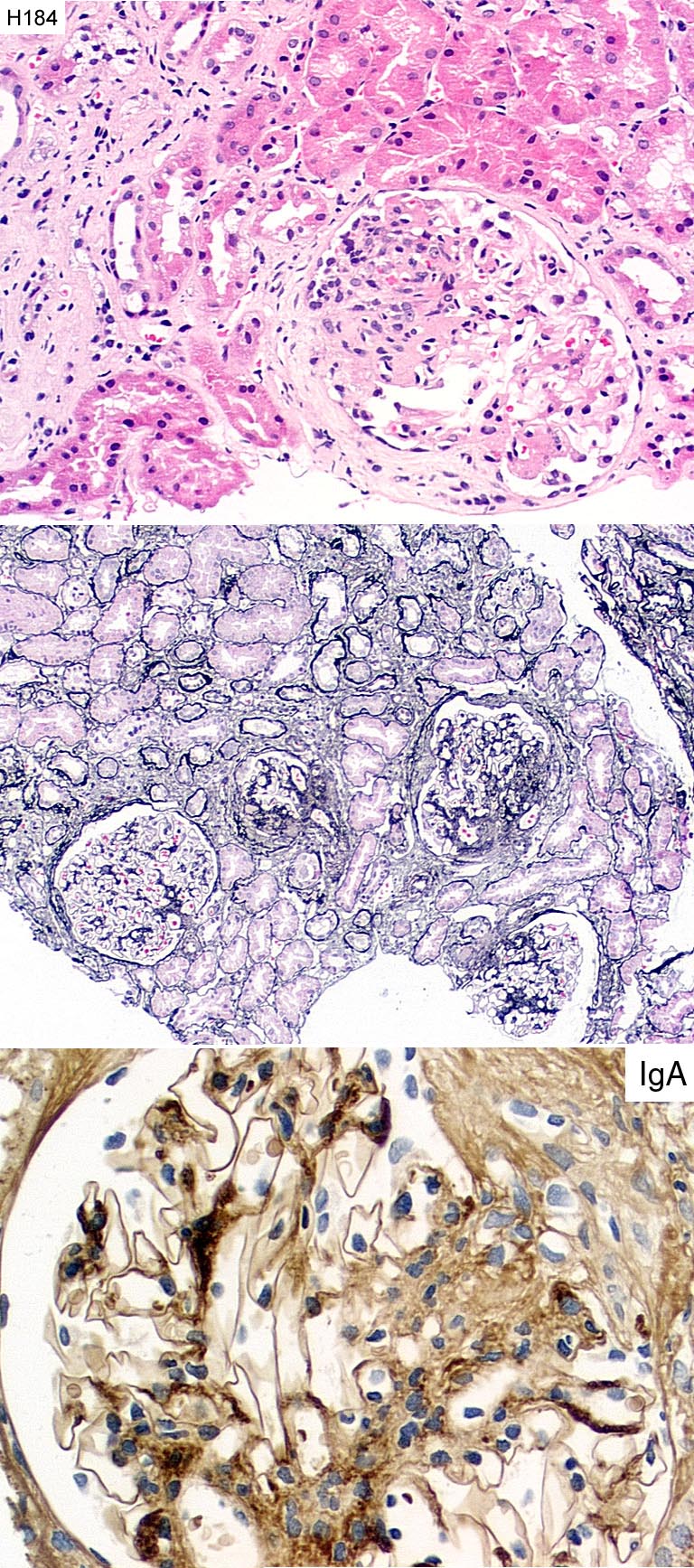
Case number: 184
....
Number of responses:75 . Date of analysis: 11 JUL 02
Clinical:
Male 41y.o. Four month history of proteinuria and microscopic haematuria.
Hypertensive. Immunoperoxidase: Diffuse mesangial C3 and IgM; IgA section
provided.
Specimen:
H&E, PA silver, IgA
Diagnostic categories: Score:
1 IgA nephropathy 9.77
2 FSGS 0.16
3 SLE 0.07
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.77
Secondary diagnoses and comments (if any):
EM*6. EVG*1. Exclude lupus*3. WHO class III*1. Type 3*1. Hypertensive
changes too*6.
Original report and further information (if any):
IgA nephropathy
Circulation: H
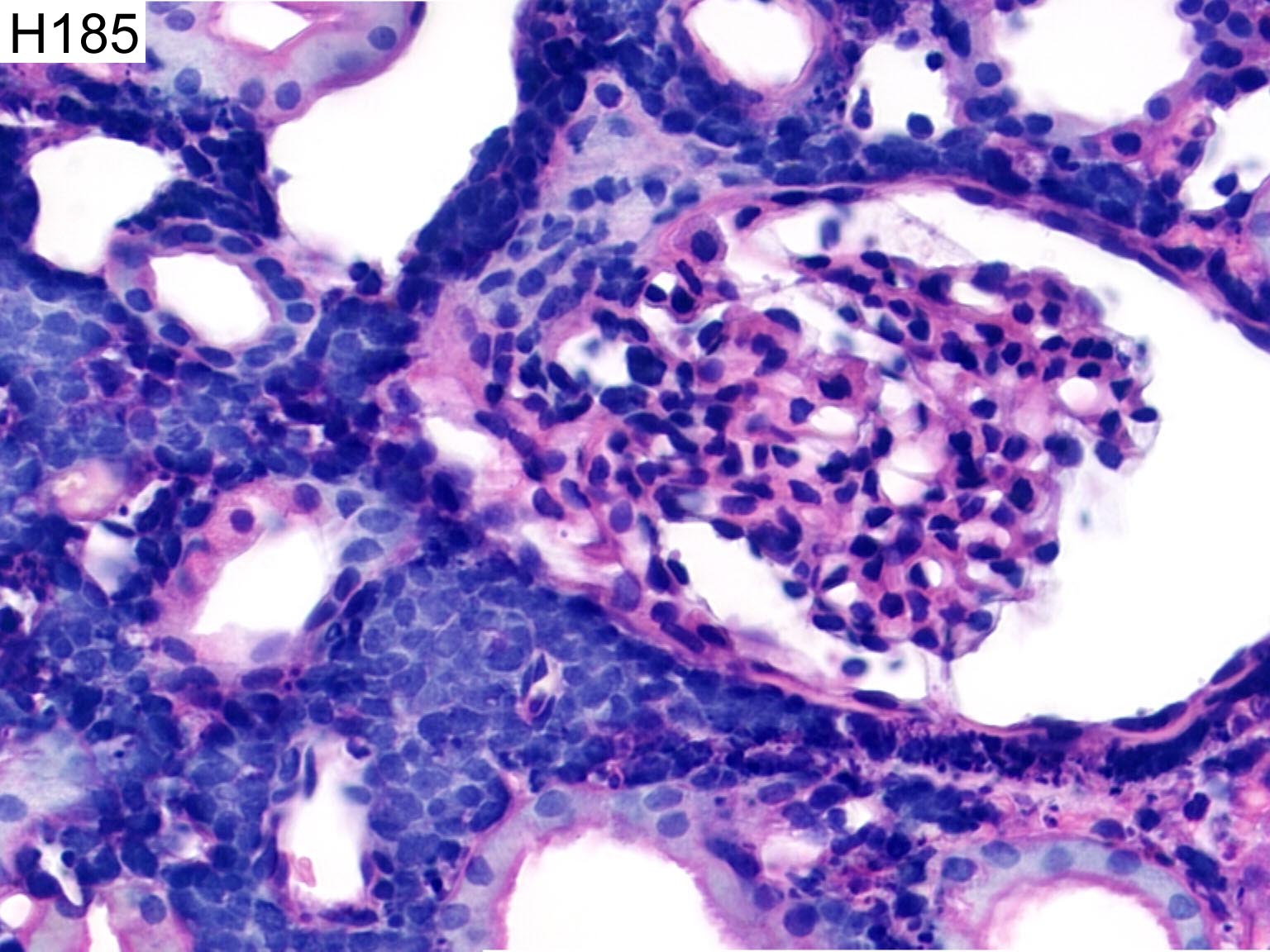
Case number: 185
....
Number of responses:75 . Date of analysis: 11 JUL 02
Clinical:
female, 43. Heart transplant 8 years ago for cardiomyopathy. 3 week history
of tingling in jaw. Platelets low, raised white cell count. Given Augmentin
for one week. Decreased urine output noted, biopsy 1 week later. No NSAIDs
given. Apologies for thin core.
Specimen:
H&E
Diagnostic categories: Score:
1 Post transplant lymphoproliferative disorder 6.43
2 Small cell carcinoma 0.03
3 Leukaemic / lymphoma infiltrate NOS 3.01
4 Malignant infiltrate, need immuno. 0.53
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.43
Secondary diagnoses and comments (if any):
Immuno for LCA*6, cytokeratin*2, lymphocyte type*33, K&L for clonality*9.
In situ/PCR for EBER/EBV*26. c-myc*1. Poor mophology (+/- rude comments)*
17. Fixed in cold tea?*1. Should be education only*3.
Original report and further information (if any):
Post-transplant lymphoproliferative disease (PTLD).
Circulation: H
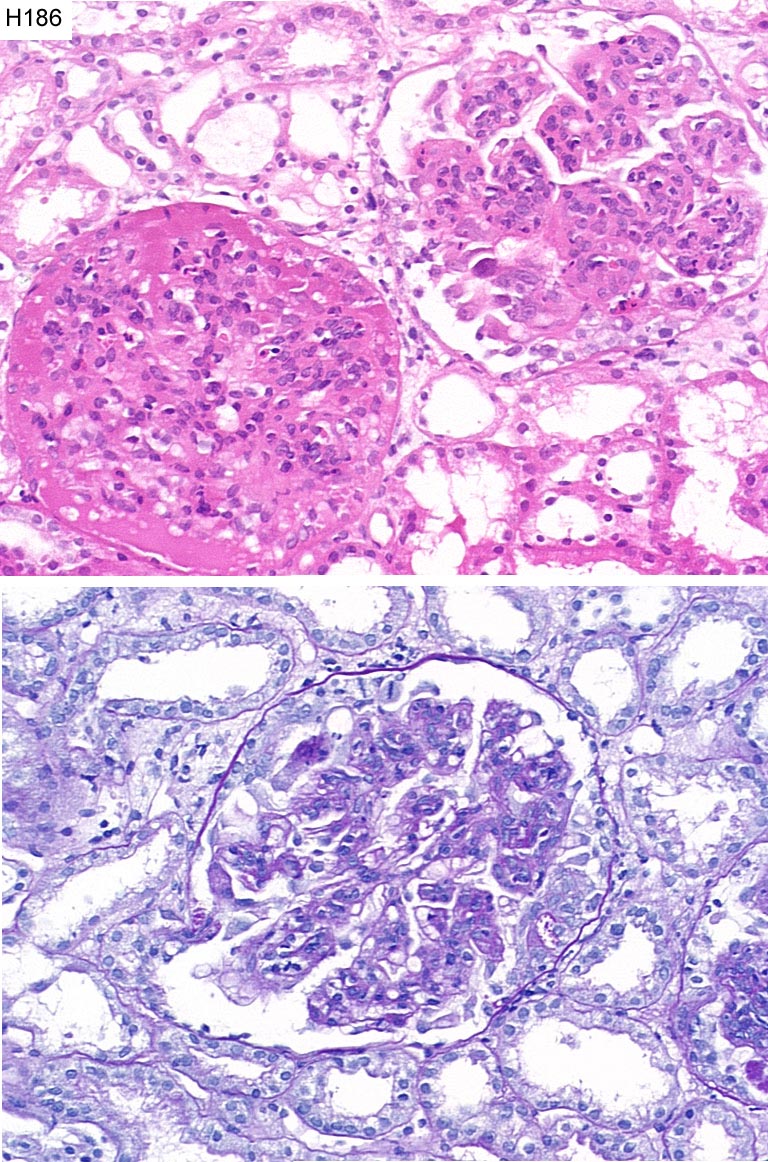
Case number: 186
....
Number of responses:75 . Date of analysis: 11 JUL 02
Clinical:
21 y.o. male. Presented with acute abdominal pain and 'vasculitic' rash.
Nephrotic range proteinuria, normal creatinine, low serum albumin, ascites
and bilateral pleural effusions. IF: moderate amounts of IgA in the
mesangium and capillary walls with smaller amounts of IgG and C3.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Henoch Schonlein Purpura 8.53
2 IgA nephropathy 0.89
3 Mesangiocapillary Gn 0.17
4 Diffuse endocapillary glomerulonephritis 0.27
10 No response 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.53
Secondary diagnoses and comments (if any):
Lupus serology*2. Silver*5. EM*6. WHO IV*1. Type 4*1. Class IIIb*1.
Circulating immune complexes?*1. Exclude infection*1.
Original report and further information (if any):
Proliferative glomerulonephritis with focal necrosis and crescent formation
consistent with Henoch-Schonlein purpura.
Circulation: H
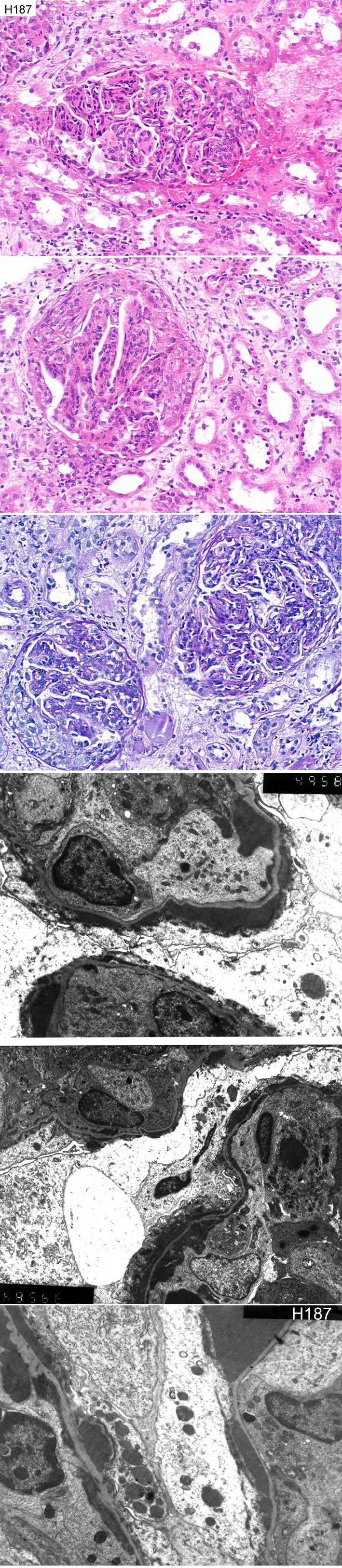
Case number: 187
....
Number of responses:75 . Date of analysis: 11 JUL 02
Clinical:
20 y.o. female. Tonsillitis 5 weeks previously. Acute nephrotic syndrome
with acute renal failure. IF: moderate to large amounts of IgG and IgM
with C3 in granular pattern glomerular capillary walls.
Specimen:
H&E, PAS, EM*3
Diagnostic categories: Score:
1 Post-strep. / endocapill. prolif. Gn 8.08
2 Acute diffuse proliferative Gn NOS 0.79
3 Lupus nephritis 0.24
4 Mesangiocapillary Gn 0.89
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.08
Secondary diagnoses and comments (if any):
Silver*4. ASOT*13. Lupus serology*9. Complement levels*2. C3nef*1. ?Family
history*1. Odd distribution of EDDs*1. EM missing*3.
Original report and further information (if any):
Crescentic glomerulonephritis with background diffuse proliferative
glomerulonephritis of endocapillary pattern
Links to cases in this document:
Top
H 182
H 183
H 184
H 185
H 186
H 187
Last updated: 11 JUL 02
Organiser:
Professor Peter Furness, PhD, FRCPath.
Clinical Sciences Laboratories
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk