National Renal Pathology E.Q.A. Scheme
Circulation C
This document gives information on individual cases in
circulation C of this scheme. It contains no personal details
of participants.
Cases included:
C 296
C 297
C 298
C 299
C 300
C 301
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: C
Case number: 296
....
Number of responses:72 . Date of analysis: 18 JUL 08
Clinical:
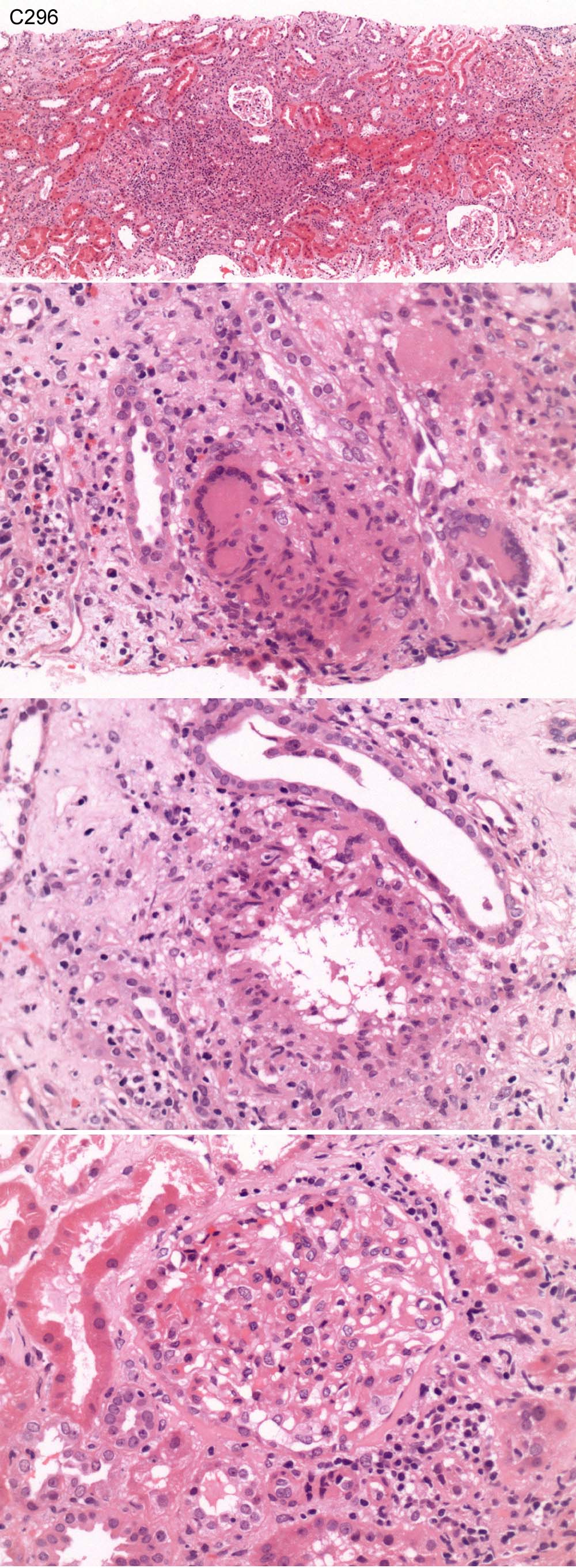
Age and sex not given. Acute renal impairment. Duplex left kidney,
previous UTI's, recently on Nitrofurantoin. Creatinine 69 in September 06,
now 350. ANA positive 1/1280, others negative. P/H TB. IF all negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Granulomatous inflammation, ?TB mentioned 2.08
2 Granulomatous inflammation ? 2ry to drugs 1.94
3 Granulomatous nephritis NOS 1.11
4 Granulomatous inflammation, differential given 3.33
5 Granulomatous nephritis ? sarcoid 0.14
6 Vasculitis 0.28
7 Tubulointerstitial nephritis NOS 1.11
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 4 with 3.33
Secondary diagnoses and comments (if any):
Z-N*27. Stains for fungi*12. Urine culture for TB*3. 2ry to drugs?*4.
Residual acute pyelonephritis?*3. Stains for fibrin*2. Lupus serology*2.
ANCA*1. Thrombophilia screen*1. FSGS-like changes in glomeruli*1. Silver/
PAS*1.
Original report and further information (if any):
Tubulionterstitial nephritis with tubulocentric granulomata, possibly
secondary to nitrofurantoin. Z-N negative. ANCA and ACE levels normal.
Circulation: C
Case number: 297
....
Number of responses:72 . Date of analysis: 18 JUL 08
Clinical:
Male, 35 years old. Previously healthy, Two month history of lower limb
swelling. Found to have normal estimated creatinine clearance but nephrotic
range proteinuria (6.5g). Negative glomerulonephritis green. Probable
FSGS. Immunoperoxidase staining for IgG and C3 showed granular positivity
within the peripheral capillary loop wall. Similar staining, although weak,
is seen with IgA. IgM is essentially negative.
Specimen:
H&E & MS x 2, EM Photos
Macro:
Two cores of tissue, both 9mm. Sample taken for Electron Microscopy.
Diagnostic categories: Score:
1 Membranous Gn 9.86
2 Membranous Gn AND FSGS 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.86
Secondary diagnoses and comments (if any):
'Negative glomerulonephritis green' really was the information given to me!
- PNF. Exclude SLE*5. Segmental glomerular changes*2. Exclude causes of
2ry membranous*1.
Original report and further information (if any):
Membranous nephropathy.
Circulation: C
Case number: 298
....
Number of responses:72 . Date of analysis: 18 JUL 08
Clinical:
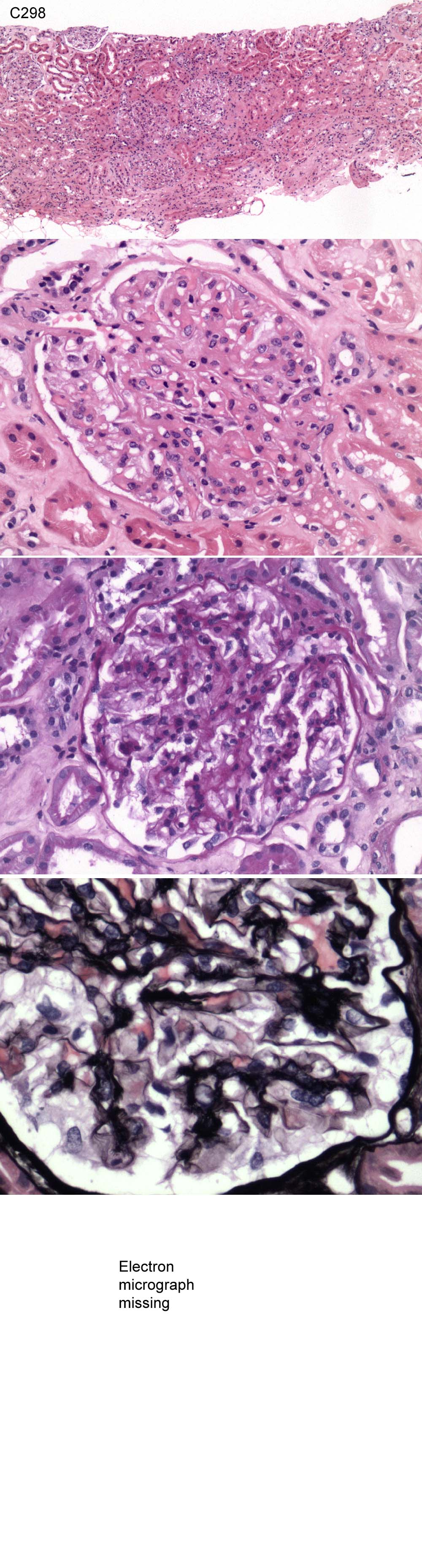
Female, 59 years. Blood and proteinuria. Previous TIA's, Cr 92. Protein
1.4g/2hr. Strong granular staining for IgG and C3 on the basement membranes
of the glomeruli on immunofluorescence, IgA, IgM, C1q negative.
Specimen:
H&E, PAS, PASM, Photo of EM
Diagnostic categories: Score:
1 Membranous Gn 9.72
2 Post-infectious Gn 0.28
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.72
Secondary diagnoses and comments (if any):
Tubular injury - exclude RVT*1. ASOT*1. Exclude secondary causes*4. Lupus
serology*2. EM*1.
Original report and further information (if any):
Circulation: C
Case number: 299
....
Number of responses:63 . Date of analysis: 18 JUL 08
Clinical:
FOR EDUCATION/INTEREST ONLY. Male, 26 years old. Presented with headaches
and severe hypertension. He was found to have nephrotic range proteinuria,
eGFR 22ml/min, Hb 10.8g/l (NR 0.75 - 1.65), C4 was normal. IF showed very
strong C3 (illustrated) but only traces of IgM. IgG, IgA and C1q were
negative.
Specimen:
H&E, Images available at http://www.pathology.plus.com/Consult/
Diagnostic categories: Score:
1 Mesangiocapillary Gn type I 2.76
2 Mesangiocapillary Gn type II 2.32
3 Mesangiocapillary Gn type III 0.63
4 Mesangiocapillary Gn type IIIb (of Strife and Anders) 0.95
5 Monoclonal Ig deposition disease 0.16
6 Mesangiocapillary Gn NOS 1.96
7 Fibrillary glomerulopathy 0.52
8 C3 nephritis 0.16
9 Light chain nephropathy 0.07
10 Diabetes, membranous, others... 0.47
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 2.76
Secondary diagnoses and comments (if any):
Congo red*1. Also hypertension *2. Relevant serology*1. Cryoglobulins*1.
More clinical info. *1. Images not accessible*6.
Original report and further information (if any):
Case discussed by NEPHNPPT international renal path. discussion group.
Consensus; McGn type IIIb (of Strife & Anders). See recent AFIP renal
fascicle. Suggested relationship to type II? Patient subsequently found to
have inherited Factor H defect.
Circulation: C
Case number: 300
....
Number of responses:72 . Date of analysis: 18 JUL 08
Clinical:
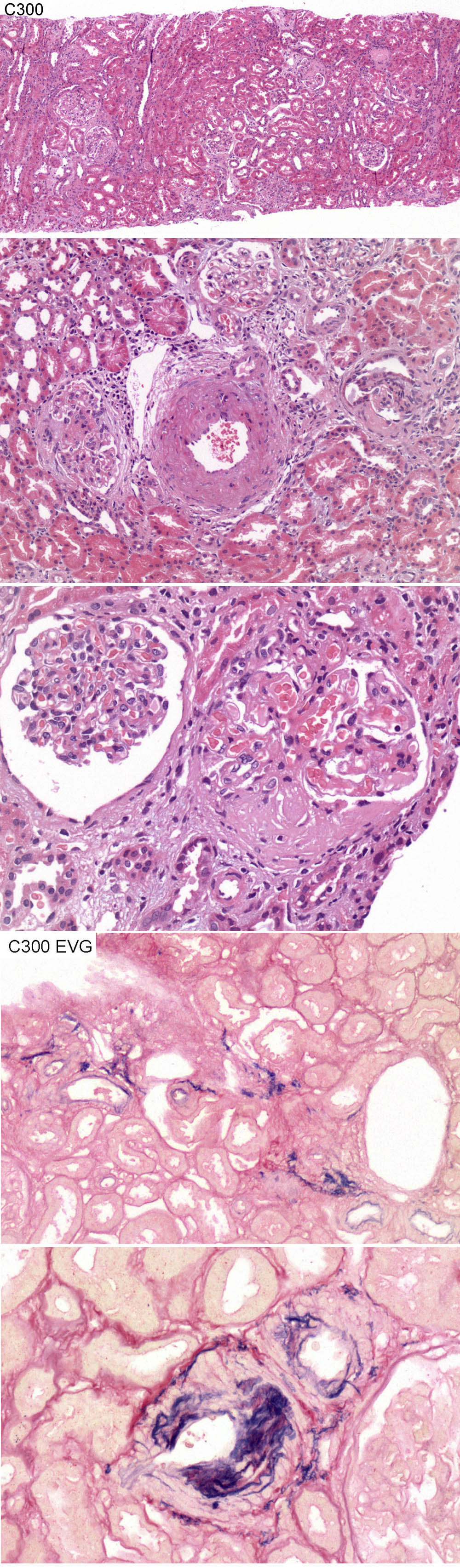
Male, 51 years old. Micro-macrohaematuria. Protein-creatinine ratio 36.
Creatinine 105. MPO positive. Intermittent ill health, treated with
courses of Prednisolone for 12 months. EM normal apart from focal tuft
collapse and wrinkling. No deposits. IF negative apart from weak diffuse
IgA, probably artefactual. CR negative.
Specimen:
H&E, Photos from EVG x 2
Diagnostic categories: Score:
1 Vasculitis (+/- quiescent / treated) 8.21
2 Focal segmental glomerulosclerosis 0.79
3 Hypertension / renovascular disease 0.86
10 Not diagnostic 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.21
Secondary diagnoses and comments (if any):
Silver*2. PAS*1. MSB*1. EM*1. MPO titre?*3. Normal range for PCR?*1. ANCA
status?*1. Clinical evidence of vasculitis?*2. ?Fabry's?*1. Levels*2. Poor
quality photos*1.
Original report and further information (if any):
Quiescent vasculitis. (Only previous treatment was prednisolone, as
stated)
Circulation: C
Case number: 301
....
Number of responses:72 . Date of analysis: 18 JUL 08
Clinical:
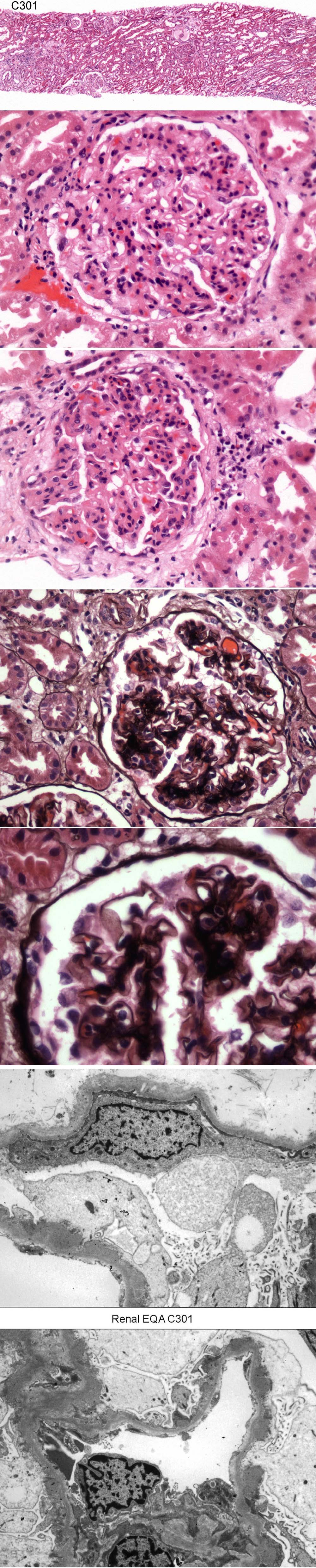
Male, 59 years old presented with proteinuria and progressive impairment of
renal function. IF showed strong granular staining for IgG and weaker
staining for IgA in a granular pattern around capillary basement membranes.
There was no staining for IgM or complement.
Specimen:
H&E, Silver, Photos of EM x 2
Diagnostic categories: Score:
1 Membranous Gn 7.94
2 Membranous Gn, probably not primary 0.14
3 Diffuse proliferative Gn 0.83
4 Membranous Gn with coexistent IgA 0.17
5 Post-infectious Gn 0.71
6 Mesangiocapillary Gn 0.21
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.94
Secondary diagnoses and comments (if any):
Membranous with some hypercellularity *4. Thick sections*9. Exclude occult
Ca, lupus, infections, other causes of 2ry membranous etc. *12. ? post-
infective Gn*2. ASO titre*1. ?diabetes too*1. Mesangial EDDs?*3.
Original report and further information (if any):
Links to cases in this document:
Top
C 296
C 297
C 298
C 299
C 300
C 301
Last updated: 18 JUL 08
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk