National Renal Pathology E.Q.A. Scheme
Circulation A
This document gives information on individual cases in
circulation A of this scheme. It contains no personal details
of participants.
Cases included:
A 284
A 285
A 286
A 287
A 288
A 289
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: A
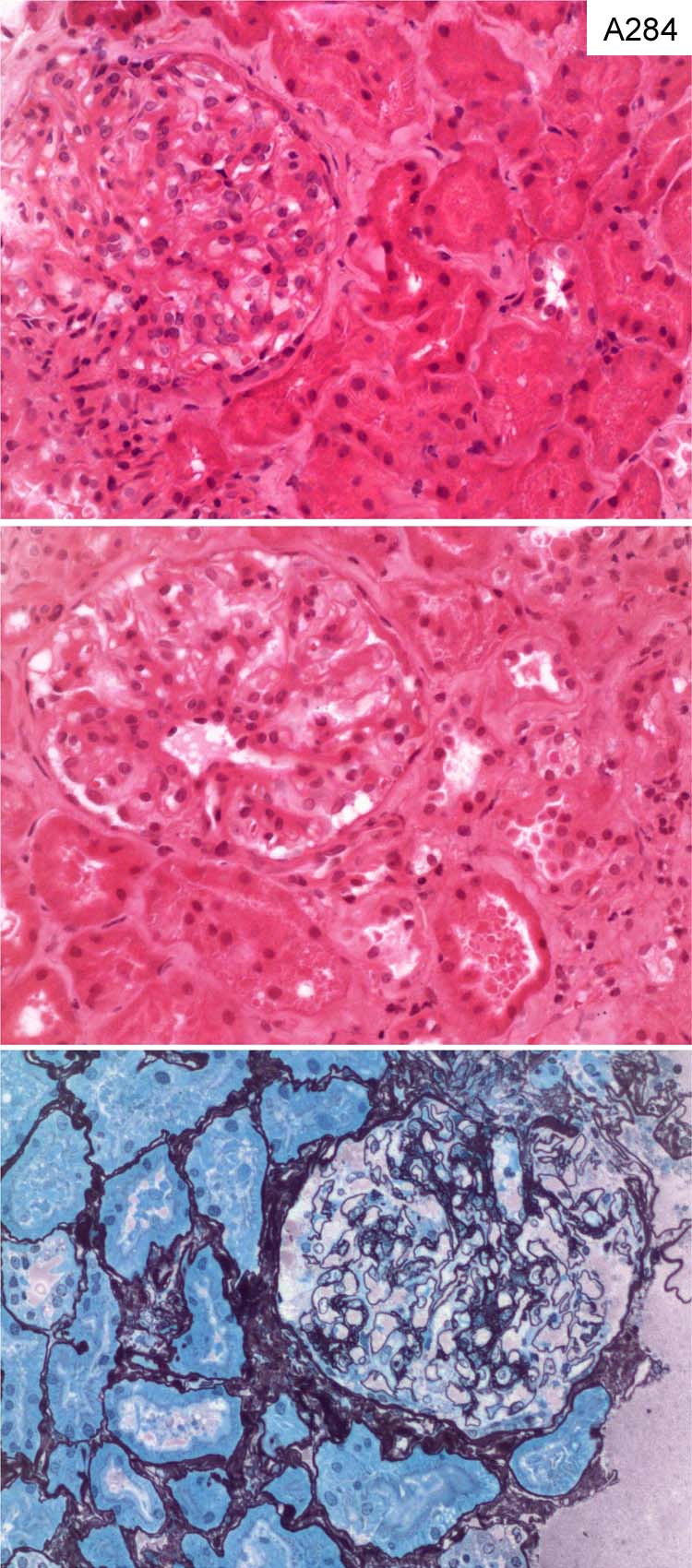
Case number: 284
....
Number of responses:78 . Date of analysis: 10 JAN 08
Clinical:
Male, 75 years old. Purpuric rash on legs, ?secondary to drugs. Blood +++,
protein ++++, protein:creatinine 257, protein concentration urine 2213.
Immunoflurescence - IgA and C3 in mesangium. Electron microscopy - deposits
in mesangium and some deposits in subendothelial zone.
Specimen:
H&E, Silver
Diagnostic categories: Score:
1 Henoch Schonlein purpura 3.08
2 IgA nephropathy 2.56
3 IgA nephropathy / HSP 4.36
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 4.36
Secondary diagnoses and comments (if any):
ATN too*1. Could rash be 2ry to drugs?*1. PAS*1. Discrepancy between
severity of clinical information and biopsy appearance?*4.
Original report and further information (if any):
Henoch-Schonlein purpura. Skin biopsy showed changes consistent with a
leukocytoclastic vasculitis.
Circulation: A
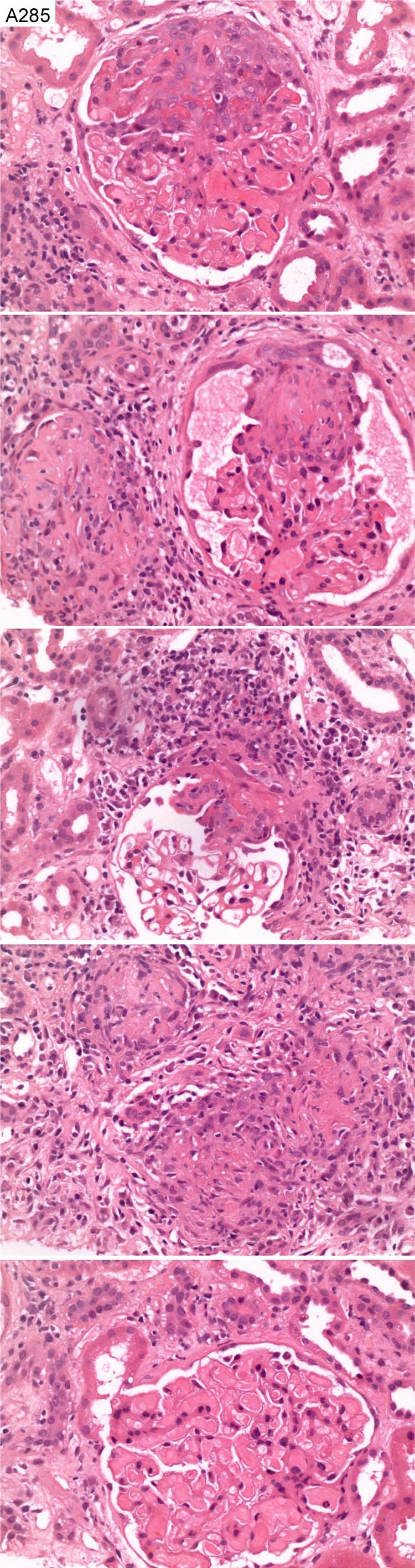
Case number: 285
....
Number of responses:78 . Date of analysis: 10 JAN 08
Clinical:
Male, 47 years old. Six months cough and blood nasal discharge.
Microscopic haematuria. Immunofluorescence showed no immunoreactants.
Specimen:
H&E
Diagnostic categories: Score:
1 Crescentic Gn c/w Wegener's 7.69
2 Pauci-immune / vasculitic crescentic Gn 2.18
3 Necrotising glomerulonephritis 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.69
Secondary diagnoses and comments (if any):
ANCA?*40. CXR*4. EM*2. Nasal biopsy*1. Silver*3. PAS*2. Congo red*1. Z-N*
1. Grocott*1. Exclude cryo*2. Anti-GBM?*4. Exclude thrombotic
microangiopathy*1. Renal function?*1. Inadequate information*1.
Original report and further information (if any):
MPO-ANCA positive, segmental necrotising GN with crescents (pauci-immune).
Circulation: A
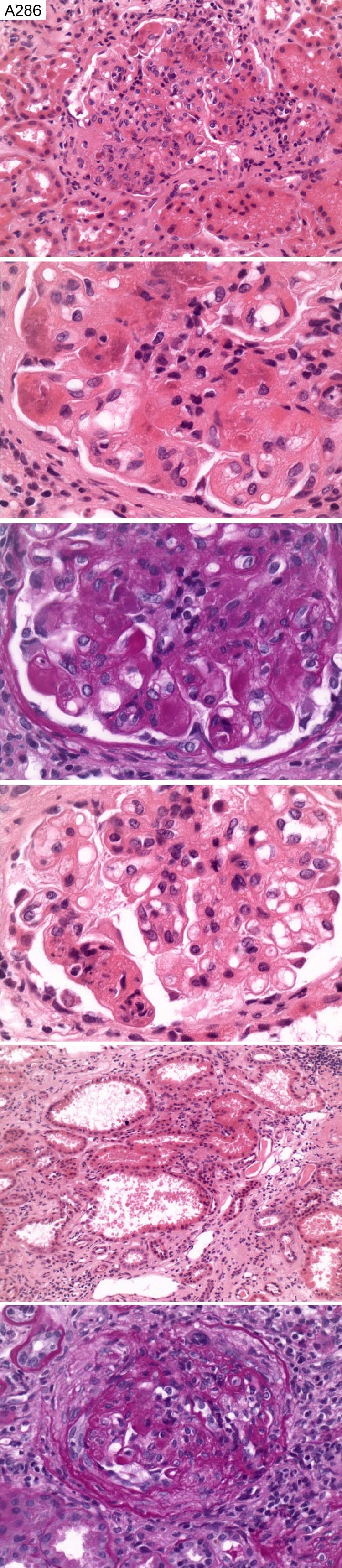
Case number: 286
....
Number of responses:78 . Date of analysis: 10 JAN 08
Clinical:
Female, 24 years old. SLE 1998. Class III biopsy 1999. Class IV Jan 2005.
On MMF > Creatinine 120 - 140. BP 145/80. Haematuria ++. Proteinuria ++.
Immunos: Glomerular as well as tubular basement membrane showed IgG (3+/4+)
IgM (2+/4+), C1q (2+/4+), C3 (4+/4+) and segmental fibrinogen (3+/4+).
Specimen:
H&E and PAS
Diagnostic categories: Score:
1 SLE class IV A/C 4.10
2 SLE class IV 2.18
3 SLE class IV A 2.31
4 SLE class IV G(A) 1.28
5 SLE class III 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 4.10
Secondary diagnoses and comments (if any):
Haematoxyphil bodies noted*2. Lupus serology*2. EM*4. Silver*4.
Insufficient glomeruli for classification*8.
Original report and further information (if any):
Class IV lupus nephritis (acute segmental necrotising glomerulonephritis).
Activity index 15/24, chronicity 8/12.
Circulation: A
Case number: 287
....
Number of responses:78 . Date of analysis: 10 JAN 08
Clinical:
Male, 61 years old. Inoperable adenocarcinoma of the pancreas, treated with
Gemcitabine. Presented with acute renal failure.
Specimen:
H&E, Photo's of silver and EM x 2
Diagnostic categories: Score:
1 HUS / thrombotic microangiopathy 6.47
2 ATN ?toxic ?HUS 0.71
3 ATN NOS 0.90
4 Oxalate nephropathy (2ry to chemo) 0.26
5 Acute tubulointerstitial nephritis 0.19
6 Mesangiocapillary Gn 0.85
7 FSGS 0.24
8 ATN and ?minimal change 0.13
9 MCGN 0.13
10 Crystal nephropathy 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.47
Secondary diagnoses and comments (if any):
Oxalate crystals noted *6. Presumably gemcitabine-related?*28. IF*2. More
clinical info.*5. Immuno. results?*7. Iscahemic changes too*1. Diabetic
changes too*1. Haematological investigation for HUS*11. Exclude tumour
lysis syndrome*1. Exclude antiphospholipid antibodies*1. Insufficient for
EQA*2.
Original report and further information (if any):
Thrombotic microangiopathy / haemolytic uraemic syndrome, probably as a
complication of gemcitabine therapy. Patient now on haemodialysis.
Circulation: A
Case number: 288
....
Number of responses:78 . Date of analysis: 10 JAN 08
Clinical:
Female, 67 years old. Nephrotic syndrome. Normal creatinine. Urine
dipstick blood + protein +++ Background - breast cancer and hypothyroid.
Specimen:
H&E, Photo's of PAS, Meth Silver and Congo Red x 2
Diagnostic categories: Score:
1 Amyloidosis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Exclude myeloma*13. Investigation for amyloid type*20. EM*3. Also ATN*1.
Original report and further information (if any):
Myeloma, confirmed by monoclonal band on electrophoresis, light chains in
urine, free lambda light chains of 363mg/l and kappa:lambda ratio of 0.03.
Bone marrow trephine confirmed yeloma. paraprotein reduced with treatment,
but still nephrotic.
Circulation: A
Case number: 289
....
Number of responses:77 . Date of analysis: 10 JAN 08
Clinical:
Sex not stated. Aged 44 years. Blood and protein in urine. Proteinuria
2.0g/day. IgA 4.3. Creatinine 80 umol/L. ANCA negative. ANA negative.
C3 and C4 normal. BP 144/85 mmHg.
Specimen:
H&E, PAAg, Photo's of IgA x 2, EM x 2
Diagnostic categories: Score:
1 IgA nephropathy 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Secondary FSGS*1. Hypertension too*1. Exclude HSP*1. Assume other IF is
negative?*4. Also chronic thrombotic microangiopathy*1.
Original report and further information (if any):
IgA mesangial proliferative glomerulonephritis, with features of focal and
segmental glomerulosclerosis.
Links to cases in this document:
Top
A 284
A 285
A 286
A 287
A 288
A 289
Last updated: 10 JAN 08
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk