National Renal Pathology E.Q.A. Scheme
Circulation W
This document gives information on individual cases in
circulation W of this scheme. It contains no personal details
of participants.
Cases included:
W 115
W 116
W 117
W 118
W 119
W 120
End
A click on the  icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: W
Case number: 115 ....
Number of responses:61 . Date of analysis: 28 JUL 98
Clinical:
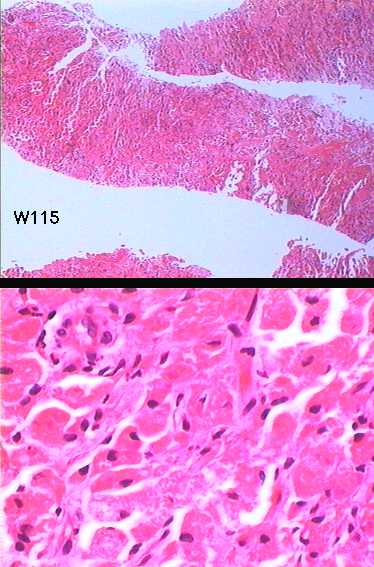
Female 72. Originally presented with right psoas abscess. Tumour arising
from lower pole right kidney. Presumed obstructing tumour with secondary
infection of 'urinoma'.
Specimen:
H&E CASE FOR INTEREST NOT EQA
Diagnostic categories: Score:
1 Renal cell carcinoma (+/- type) 2.31
2 Oncocytoma 1.49
3 Malacoplakia 4.54
4 Xanthogranulomatous pyelonephritis 0.80
5 Granular cell tumour 0.33
6 Angiomyolipoma 0.10
7 Transitional cell carcinoma 0.16
8 Megalocytic interstitial nephritis 0.16
9 Epithelioid leiomyosarcoma 0.07
10 Rhabdomyosarcoma 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 4.54
Secondary diagnoses and comments (if any):
Need immuno for cell type*12. Stain to confirm ? Michaelis-Gutmann
bodies*11. E.M.*4. ZN*1. Need resection for confirmation*2. Urine
culture*1. Material too degenerate for diagnosis *1.
Original report and further information (if any):
Malakoplakia.
Peri-renal haematoma after biopsy (on warfarin!). No surgery due to cardiac
and peripheral vascular problems. Died 6 months later of myocardial
infarction.
Circulation: W
Case number: 116 ....
Number of responses:64 . Date of analysis: 28 JUL 98
Clinical:
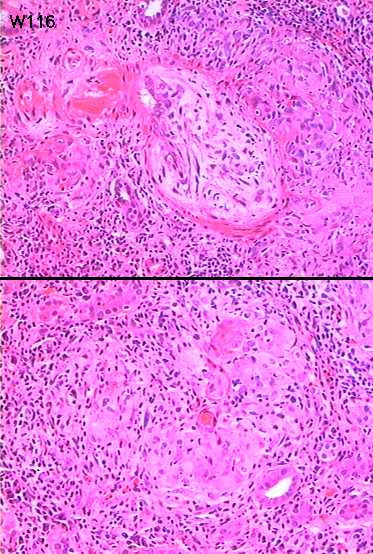
Male 44. History of nephritis in childhood. Now has haematuria and
proteinuria, creatinine 220 and erythema nodosum.
Specimen:
H&E
Diagnostic categories: Score:
1 Granulomatous interstitial nephritis +/- differential 7.50
2 Sarcoidosis 1.09
3 Wegeners granulomatosis 0.67
4 PAN / vasculitis NOS 0.48
5 Churg-Strauss syndrome 0.16
6 Tuberculosis 0.06
7 Granulomatous drug reaction 0.03
10 (Diagnosis merging will clearly be needed! - PF) 0.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.50
Secondary diagnoses and comments (if any):
?sarcoid / ?ACE levels*27. ?drug reaction*15. ?TB / Z-N*22. ?infection*4.
?Crohn's*3. Stains for fungi*6. ANCA/?Wegener's*19. Churg-Strauss*2. IF*
2. Silver stain*1. Elastin*2. MSB*1. Levels*1.
Original report and further information (if any):
Granulomatous tubulo-interstitial nephritis, probably sarcoid.
Subsequently reponded to steroids. Clinically appeared to be sarcoid.
Circulation: W
Case number: 117 ....
Number of responses:64 . Date of analysis: 28 JUL 98
Clinical:
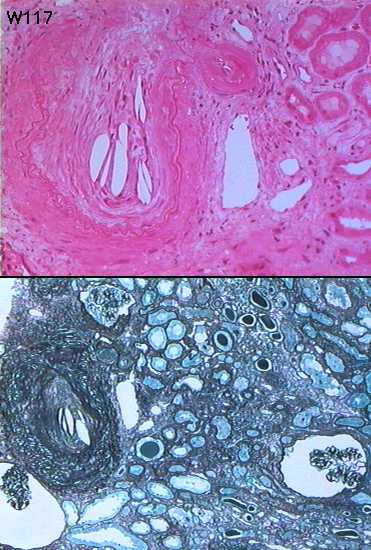
73 y.o. man with non-insulin dependent diabetes mellitus and previous aortic
aneurysm repair. Proteinuria ++, raised creatinine and peripheral
eosinophilia. Provisional diagnosis of renovascular disease. IF: linear
IgG + in capillary walls of viable glomeruli, patchy non-specific IgM and C3
Specimen:
H&E and silver
Diagnostic categories: Score:
1 Cholesterol / atherosclerotic emboli 9.06
2 Ischaemic damage / vascular disease NOS 0.63
3 Membranous glomerulonephritis 0.16
4 Diabetes 0.09
5 Anti-GBM disease 0.03
6 Lupus 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.06
Secondary diagnoses and comments (if any):
Infarction noted*1. Diabetic changes too*16. No diabetic changes*6. Relates
to AAA repair*4. Need to see IF*2. Need EM*4. IgG presumably artefactual /
diabetic?*6. Membranous Gn too*1. ?amyloid too*1. ?light chain nephropathy
too*1. Membranous glomerulonephritis too*1. Poor section*1.
Original report and further information (if any):
Cholesterol (atheromatous) embolism. Subsequently lost to follow up.
Circulation: W
Case number: 118 ....
Number of responses:64 . Date of analysis: 28 JUL 98
Clinical:
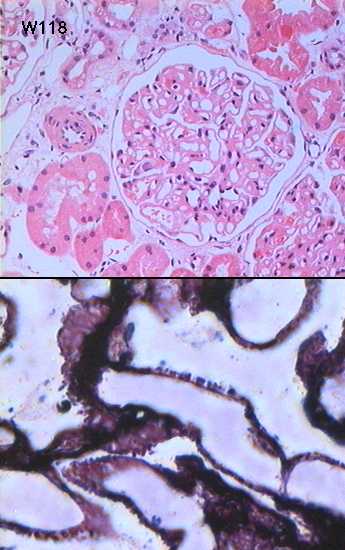
56 y.o. woman, proteinuria over 1g/day. Congo red negative. IF: peripheral
granular C3, weak peripheral granular IgG. E.M.: thickening of glomerular
basement membrane with scattered epimembranous deposits.
Specimen:
H&E, Silver
Diagnostic categories: Score:
1 Membranous glomerulonephritis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Vascular changes too*2. ?SLE related*1. Exclude secondary causes *1. Stain
for amyloid *1. Why no deposits on EM?*2.
Original report and further information (if any):
Membranous glomerulonephritis.
Circulation: W
Case number: 119 ....
Number of responses:57 . Date of analysis: 28 JUL 98
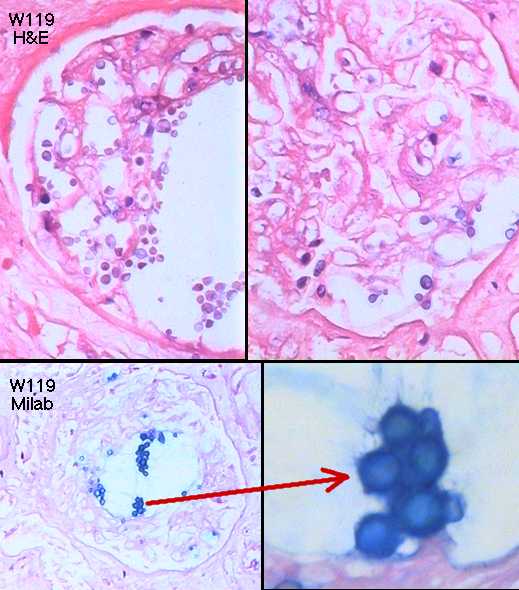
Clinical:
59 y.o. male. Autopsy kidney. Cardiac transplant 4 years previously.
Recently treated for vascular rejection. CASE FOR EDUCATION NOT PERSONAL
ASSESSMENT
Specimen:
H&E & Milab
Diagnostic categories: Score:
1 Fungal / parasitic infection NOS 1.93
2 Cryptococcosis 6.32
3 Candida 0.53
4 Pneumocystis 0.18
5 Chronic rejection 0.18
6 Lymphoma / PTLD 0.53
7 Infarction NOS 0.18
8 Torulopsosis 0.09
9 CMV 0.09
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.32
Secondary diagnoses and comments (if any):
Hypertension*1. ?CyA effect on vessels*2. Severe autolysis*2. Fungi=
overgrowth?*1. Focal segmental Gn too*1.
What's a Milab?*8. (Apparently it's not 'Milab's stain for cryptococcus'
- it's Miller's Alcian Blue -PF)
Original report and further information (if any):
Cryptococcus septicaemia secondary to immunosuppression.
Circulation: W
Case number: 120 ....
Number of responses:62 . Date of analysis: 28 JUL 98
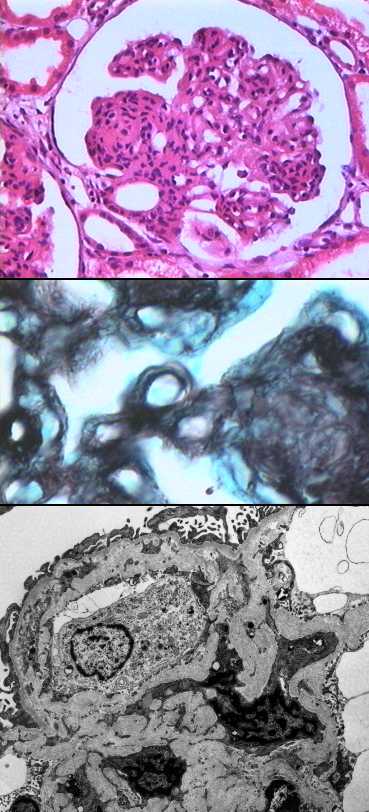
Clinical:
26 y.o. female. Explanted kidney not used for transplantation. Donor died
from subarachnoid haemorrhage. No tissue available for IF.
Specimen:
H&E, MST, PAS, E.M.x2
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis 8.31
2 Lobular / mesangiocapillary glomerulonephritis 0.37
3 Endocapillary / post-strep. glomerulonephritis 0.05
4 Mesangial proliferative glomerulonephritis 0.31
5 Diabetic glomerulosclerosis 0.26
6 Diffuse proliferative glomerulonephritis 0.16
7 Hypertension / chronic vascular disease NOS 0.23
8 Scleroderma 0.16
10 Don't know / no answer 0.16
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.31
Secondary diagnoses and comments (if any):
MCGn Type I *9. Why no deposits on EM?*8. Exclude scleroderma*2. Exclude
diabetes*2. Exclude infection*1. Exclude SLE*5. Pre-eclampsia?*1.
Paraproteins?*1. Immunoperoxidase*5. Hypertension too*1. 'tubular
dystrophy' too*1.
Original report and further information (if any):
Mesangiocapillary glomerulonephritis
Links to cases in this document:
Top
W 115
W 116
W 117
W 118
W 119
W 120
Last updated: 28 JUL 98
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk