National Renal Pathology E.Q.A. Scheme
Circulation T
This document gives information on individual cases in
circulation T of this scheme. It contains no personal details
of participants.
Cases included:
T 97
T 98
T 99
T 100
T 101
T 102
End
A click on the  icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
icon should provide an image from the material circulated. Some of the
images are composites - remember to scroll the image to see parts beyond the bottom
of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as a 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: T
Case number: 97 ....
Number of responses:44 . Date of analysis: 16 DEC 97
Clinical:
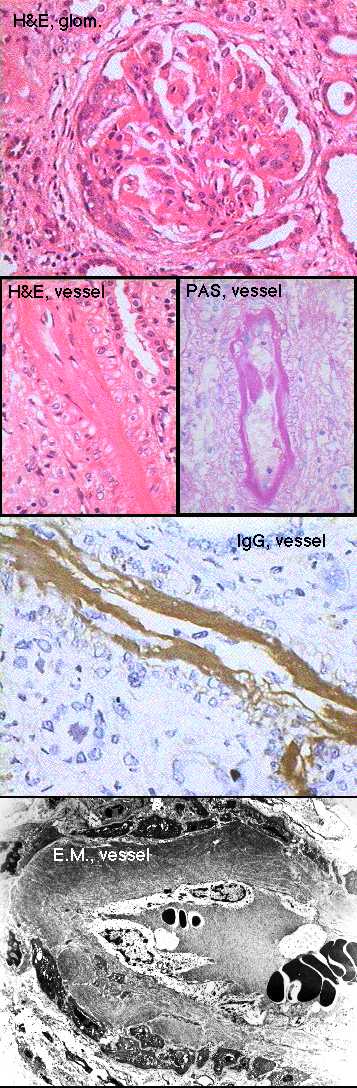
DIFFICULT CASE FOR DISCUSSION, NOT PERSONAL ASSESSMENT Male, born 1973.
Intestinal lymphangiectasia diagnosed 1989 (H&E also included). Further
clinical details on attached note; nephrotic & impaired renal function,
responded to cyclophosphamide. Any definite diagnoses to Dr Howat (Preston)
Specimen:
H&E, PAS, silver, IgG, A, M, C3, C1q, EMX3.
Diagnostic categories: Score:
1 Crescentic glomerulonephritis NOS 0.68
2 Cryoglobulinaemia / paraproteinaemia 2.09
3 Mesangiocapillary glomerulonephritis 3.45
4 Henoch - Schonlein 0.11
5 Fibrillary / immunotactoid glomerulonephritis 0.50
6 Amyloid-like material 0.23
7 Lupus or similar (even if seronegative) 0.70
8 Microangiopathy 0.18
9 Immune complex glomerulonephritis NOS 0.23
10 G.O.K. etc. 1.82
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 3.45
Secondary diagnoses and comments (if any):
Immunoelectrophoresis *5. Bone marrow*1. ?SLE*8. More clinical info*1.
Vasculitis elsewhere?*1. Family history?*1. Hepatitis (C) status?*3. Are
deposits light-chain restricted?*1.
Glomerular changes in lymph blockage; see Gastroent. 48:642(1965) & JTr Med
Hyg 82:150(1979).
Original report and further information (if any):
See letter from Dr Howat. Initial recovery after cyclophosphamide but
subsequent decline to CRF. On CAPD, awaiting transplant. Subsequenty had
grand mal fits and occipital infarct.
Circulation: T
Case number: 98 ....
Number of responses:69 . Date of analysis: 16 DEC 97
Clinical:
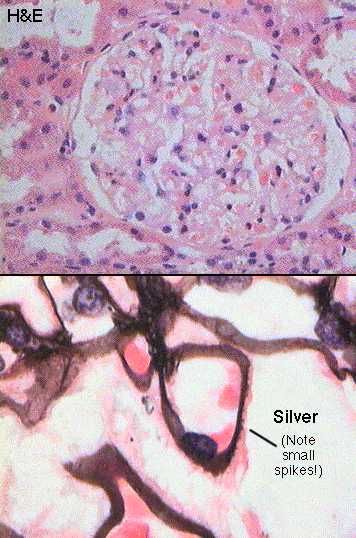
37 y.o. man, presented with nephrotic syndrome. No medication. Normal renal
function. IF: strong granular IgG round basement membranes, weaker IgM and
complement, IgA negative. E.M.: subepithelial dense deposits.
Specimen:
H&E, silver
Diagnostic categories: Score:
1 Membranous glomerulonephritis 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Hypertension too*2.
Original report and further information (if any):
Membranous glomerulonephritis.
Circulation: T
Case number: 99 ....
Number of responses:69 . Date of analysis: 16 DEC 97
Clinical:
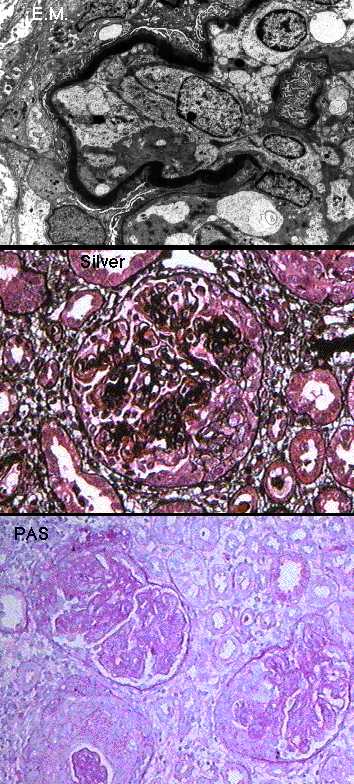
7y.o. boy , 2 weeks history of upper respiratory tract infection followed by
nephritic picture , 4+ blood and protein in urine. IF: segmental C3 , 2+ in
capillary walls and 3+ mesangium. Immunoglobulins virtually negative.
Specimen:
PAS, PASM, MSB (H&E not supplied). EM x 2.
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis type II 7.64
2 Post-streptococcal / acute diffuse prolif. Gn 1.64
3 Rapidly progressive / crescentic glomerulonephritis 0.72
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.64
Secondary diagnoses and comments (if any):
ANCA?*1. ASOT*4. Serum C3*1. Any C3 in TMBs?*1. C3Nef?*3.
Lipodystrophy?*3. H&E please!*2.
Original report and further information (if any):
Rapidly progressive sclerotic and crescentic glomerulonephritis. Type II
mesangiocapillary (DDD) among a few other nephritides could produce this
picture.
Further report when E.M. available: Diagnostic of type II
mesangiocapillary glomerulonephritis.
Circulation: T
Case number: 100 ....
Number of responses:69 . Date of analysis: 16 DEC 97
Clinical:
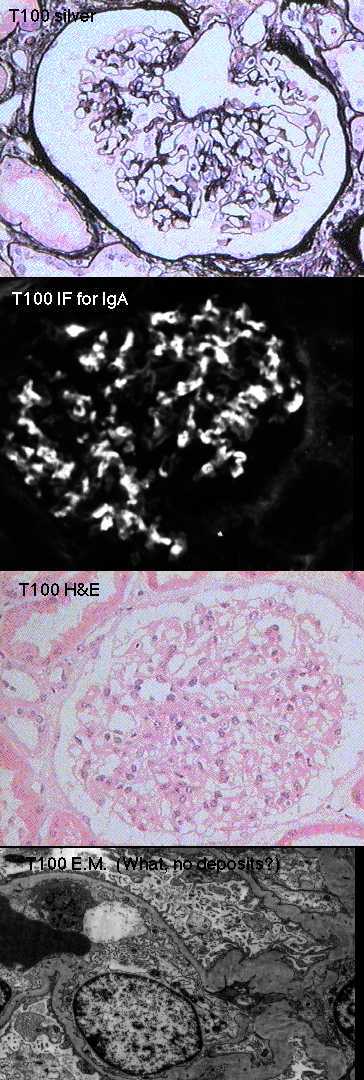
74y.o. man, hypertensive for 10 years, vasculitic rash thighs, buttocks and
elbows. Deteriorating renal function. Creatinine 168 to 190um/l over 4 days.
protein 0.4g/24h. Blood ++. BP 180/120. C3 similar to IgA, other IF
negative.
Specimen:
H&E, Meth. silver, photo of IgA*2, e.m.*2
Diagnostic categories: Score:
1 Henoch Schonelin purpura / IgA nephropathy 9.83
2 Proliferative glomerulonephritis 0.14
3 Vasculitis 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.83
Secondary diagnoses and comments (if any):
Review e.m. for deposits *4. Hypertension too*8. Exclude SLE*3. ATN too*1.
Too old for HSP*2. Skin Bx.*1.
Original report and further information (if any):
Circulation: T
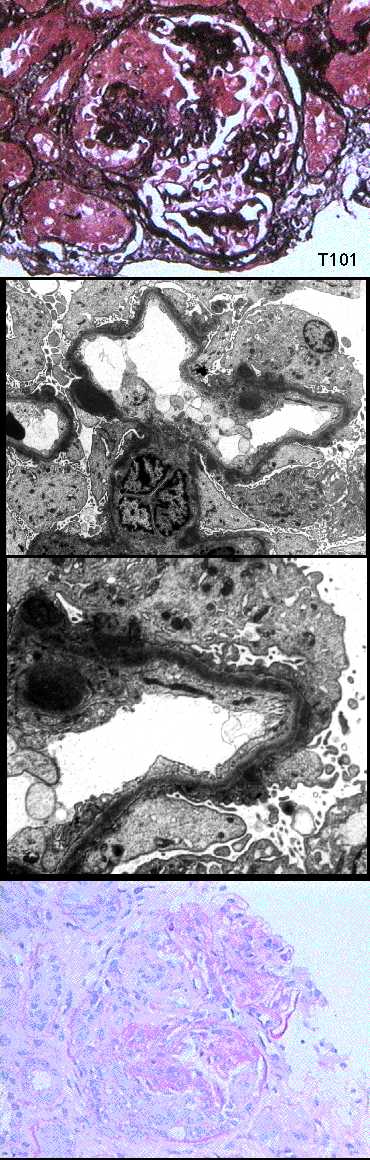
Case number: 101 ....
Number of responses:69 . Date of analysis: 16 DEC 97
Clinical:
10y.o. female, presented with microhaematuria, proteinuria, ascites, oedema.
IF: segmental trace IgG in capillary walls, 1+ in mesangium; C3 1+ to 2+
in capillary walls and mesangium; IgA, IgM negative.
Specimen:
PAS, PASM, MSB, E.M.x1. No H&E.
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis 2.74
2 Acute diffuse / post-strep Gn 5.59
3 Crescentic glomerulonephritis NOS 1.38
4 Membranous nephropathy (with crescents) ? due to lupus 0.14
5 Henoch Schonlein syndrome 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 5.59
Secondary diagnoses and comments (if any):
Crescents noted*7. Exclude lupus*3. ASOT?*10. Sore throat?*4. Serum C3?*
2. C3nef?*1. Exclude SBE*1.
'Humps' unusual but have been reported in dense deposit disease*1.
Complaints about no H&E*4.
Original report and further information (if any):
Diffuse endocapillary proliferative (post-infectious) glomerulonephritis
with crescents.
Circulation: T
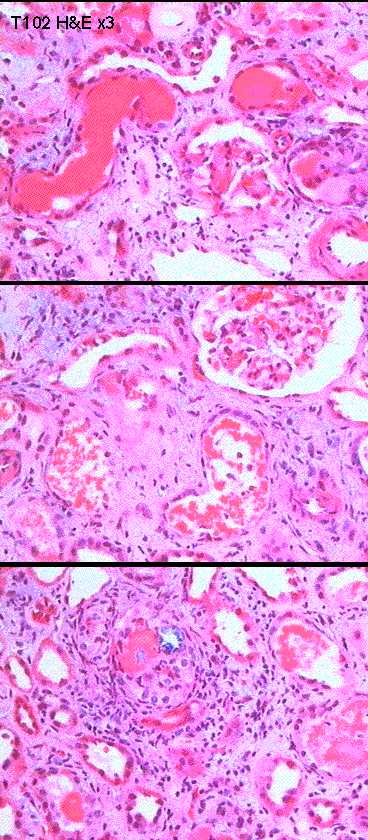
Case number: 102 ....
Number of responses:68 . Date of analysis: 16 DEC 97
Clinical:
Male of 68. Acute renal failure. patient has paraproteinaemia. IF
negative.
Specimen:
H&E
Diagnostic categories: Score:
1 Myeloma kidney 9.16
2 Amyloid 0.29
3 Interstitial nephritis 0.25
4 Light chain nephropathy 0.29
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.16
Secondary diagnoses and comments (if any):
Congo red*8. Kappa & lambda *2. Bone marrow*2. Radiology*1. E.M. *1.
PAS*1. ATN too*3. Exclude cryo*1.
Original report and further information (if any):
Myeloma kidney.
Links to cases in this document:
Top
T 97
T 98
T 99
T 100
T 101
T 102
 Home Page
Home Page
 CWIS
CWIS
 Pathology EQA
Pathology EQA
Last updated: 16 DEC 97
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582 Fax: (0116) 2584573
Email: pnf1@le.ac.uk