National Renal Pathology E.Q.A. Scheme
Circulation L
This document gives information on individual cases in
circulation L of this scheme. It contains no personal details
of participants.
Cases included:
L 200
L 201
L 202
L 203
L 204
L 205
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: L
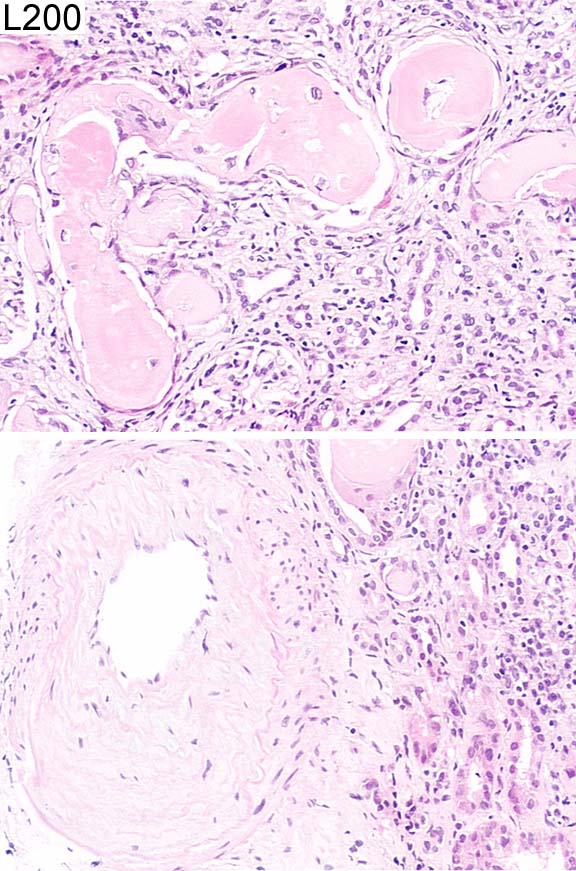
Case number: 200
....
Number of responses:74 . Date of analysis: 27 APR 03
Clinical:
67 year old woman with blood and proteinuria, renal bruit, raised creatinine
and calcium.
Specimen:
H&E, PAS
Diagnostic categories: Score:
1 Myeloma cast nephropathy 9.19
2 Chronic vascular disease (exclude myeloma) 0.27
3 Renal artery stenosis / benign nephrosclerosis 0.41
4 IgA nephropathy 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.19
Secondary diagnoses and comments (if any):
Chronic vascular disease too*15. Interstitial inflammation*2. IF*1. EM*2.
Bence-Jones protein?*8. Immunoelectrophoresis*20. Marrow aspirate*2. K and
L immunohisto.*4. Exclude lymphoid neoplasia*1. Acute TIN too*2. Congo
red*7. Staining too pale*2.
Original report and further information (if any):
Myeloma kidney. Found to have monoclonal IgA kappa paraprotein, 'pepper-
pot' skull and 41% plasma cells in bone marrow aspirate. Did not respond
to treatment; died a few months later.
Circulation: L
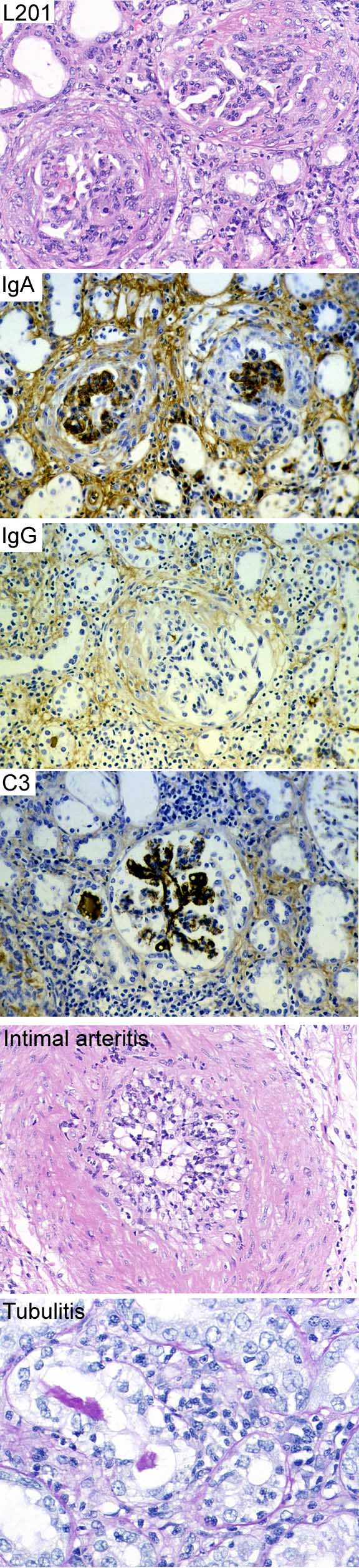
Case number: 201
....
Number of responses:65 . Date of analysis: 27 APR 03
Clinical:
54 year old man. Rejected transplant kidney. Transplanted 5 years ago for
glomerulonephritis. Failed recently ?recurrence of original disease. For
Educational Interest only.
Specimen:
H&E, PAS. IgA, IgG, C3
Diagnostic categories: Score:
1 Recurrent IgA nephropathy 2.31
2 Recurrent IgAN AND acute rejection 6.00
3 Chronic vascular rejection 0.15
4 Crescentic glomerulonephritis and vasculitis 0.15
5 Recurrent IgAN AND chronic rejection 1.08
6 SLE 0.15
7 Crescentic glomerulonephritis and rejection 0.15
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.00
Secondary diagnoses and comments (if any):
Presumably immunosuppression stopped before nephrectomy?*5. Transplant
glomerulopathy*2. ?polyoma virus too*1. What was original disease?*6.
Original report and further information (if any):
Recurrent IgA nephropathy, with crescents. Also severe acute rejection (
due to cessation of immunosuppression prior to graft nephrectomy).
Circulation: L
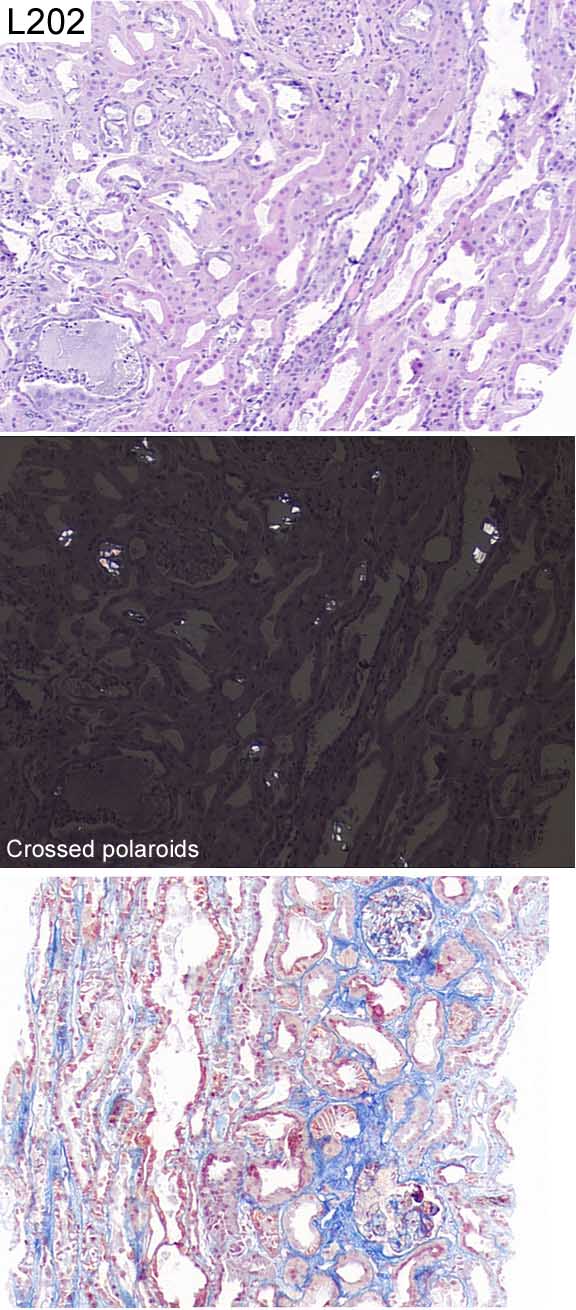
Case number: 202
....
Number of responses:74 . Date of analysis: 27 APR 03
Clinical:
71 year old male; history of chronic alcohol abuse; acute renal failure with
anuria and haemodialysis; microhaematuria; leucocyturia.
Specimen:
H&E, Trichrome (AFOG)
Diagnostic categories: Score:
1 Crystal nephropathy, Ethylene glycol mentioned 6.62
2 Crystal nephropathy NOS 0.14
3 ATN, crystals not mentioned 0.14
4 Oxalate crystal nephropathy 2.57
5 Microangiopathy / HUS 0.14
6 Gouty nephropathy / uric acid crystals 0.14
7 Oxalate nephropathy AND mesangiocapillary Gn 0.14
8 Acute urate nephropathy 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.62
Secondary diagnoses and comments (if any):
Liver function?*1. Also membranous Gn*1. Silver stain*2. EM*2. IF*2.
Exclude cryoglobulin*1.
Original report and further information (if any):
Oxalosis due to ethylene glycol ingestion.
Circulation: L
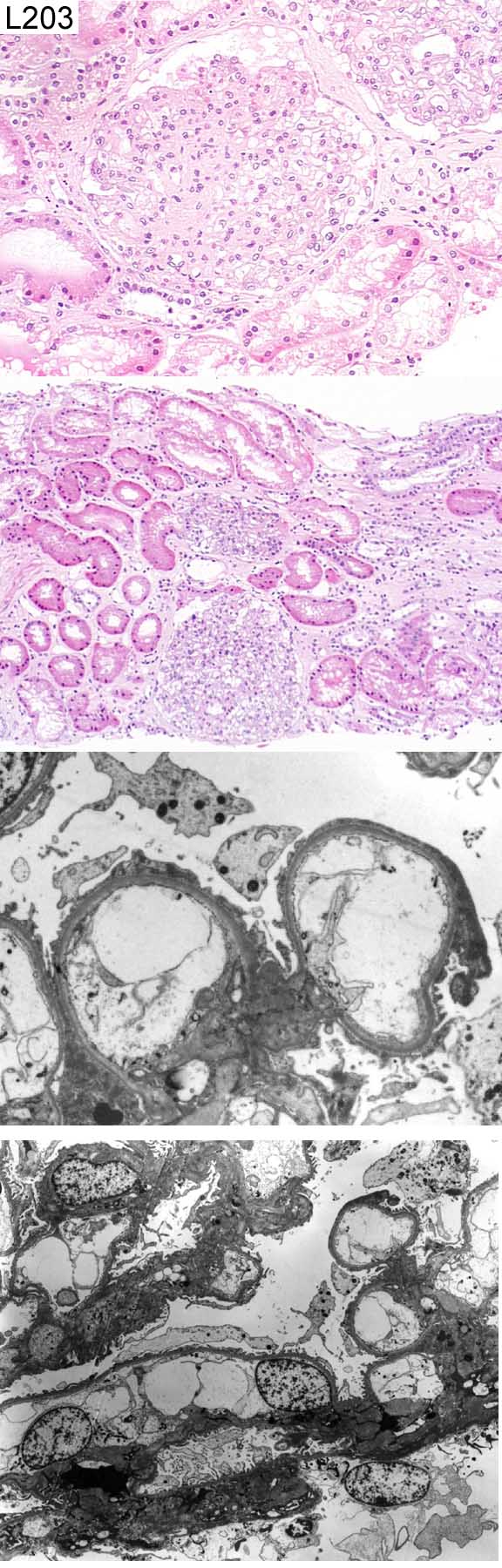
Case number: 203
....
Number of responses:74 . Date of analysis: 27 APR 03
Clinical:
Male, 35 years. Incidental finding of haematuria and proteinuria. The
patient did not have hypertension or diabetes mellitus. 24 hour urine
protein 2.8g, blood urea 4.9 mmol/l, creatinine 106 umol/l. Urine
dysmorphic red blood cells positive. Direct immunofluorescence study is
negative for IgG, IgA, IgM, C3 and C1q
Specimen:
H&E, EM*1
Diagnostic categories: Score:
1 Focal segmental glomerulosclerosis 5.44
2 Inherited GBM abnormality (+/- 2ry FSGS) 2.36
3 Mesangial proliferative glomerulonephritis 0.72
4 Pauci-immune RPGn 0.14
5 Lipoprotein abnormality (various) 0.41
6 Sickle cell disease 0.14
7 Fat embolus 0.14
8 Microangiopathy / HUS 0.41
9 Mesangiocapillary Gn 0.14
10 Don't know 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.44
Secondary diagnoses and comments (if any):
Silver*6. PAS*2. Higher mag. EM*9. BM thickness?*5. Repeat IF*2. IF for
light chains*1. Family history?*5. Norwegian?*1. Obese?*1. HIV?*2. SLE
serology?*1. Oligomeganephronia?*1. Perl's stain*1. Trichrome*1.
Unsuitable for EQA*5.
Original report and further information (if any):
Primary focal segmental glomerulosclerosis.
Circulation: L
Case number: 204
....
Number of responses:74 . Date of analysis: 27 APR 03
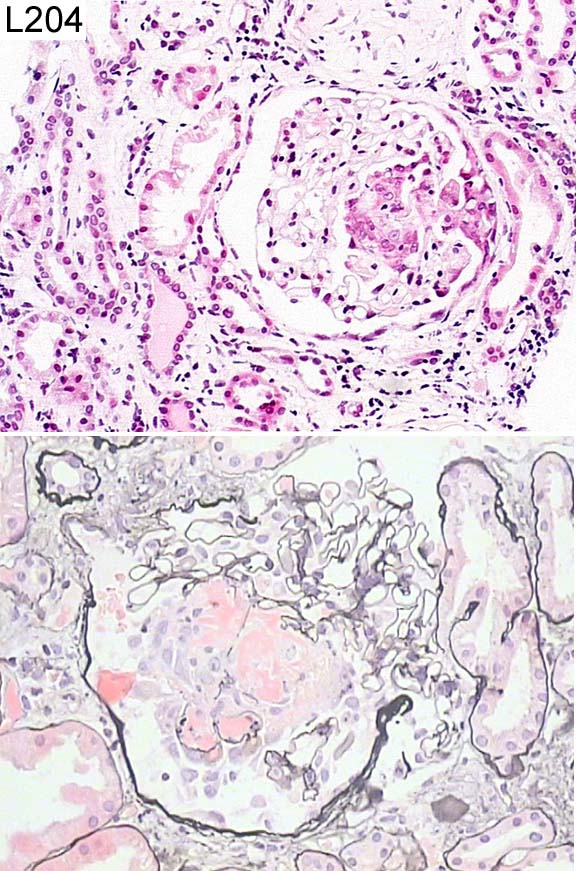
Clinical:
71 year old female. Mild hypertension, creatinine 183 umol/l, MPO positive
(138), ultrasound scan - both kidneys 8.5cm. ?Vasculitis. ?Membranous. ?
IgA. Immunohistochemistry for IgA, IgG, IgM and Complement are negative. EM
not undertaken.
Specimen:
H&E, Image of PAS
Diagnostic categories: Score:
1 Pauci-immune necrotising Gn / vasculitis 9.05
2 Focal necrotising Gn 0.68
3 Crescentic Gn 0.14
4 Interstitial nephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.05
Secondary diagnoses and comments (if any):
ANCA?*5. Lupus serology?*1. H&E too pale*14.
Original report and further information (if any):
Focal segmental necrotising glomeruonephritis. Subsequent
immunohistochemistry showed only non-specific positivity. Final
conclusion: Consistent with vasculitic process.
Circulation: L
Case number: 205
....
Number of responses:73 . Date of analysis: 27 APR 03
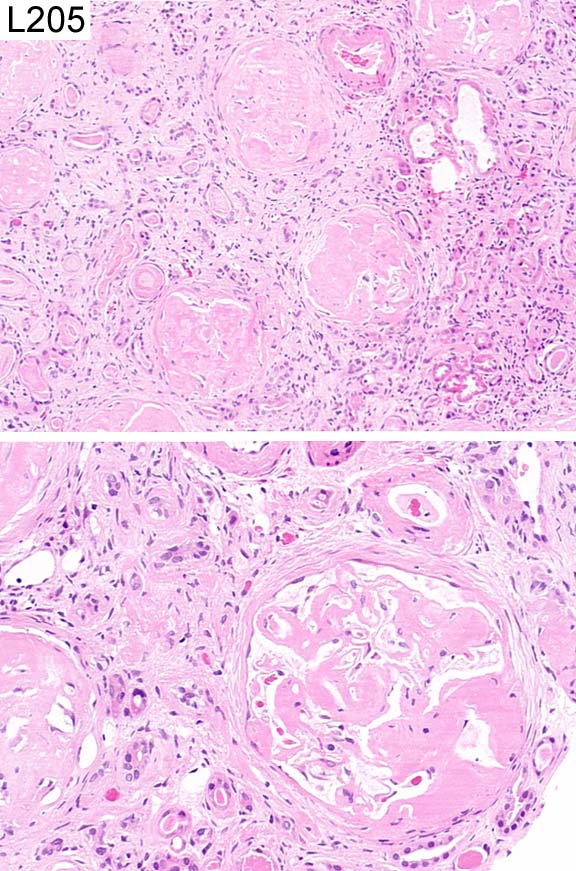
Clinical:
Male, 70 years with Waldenstroms macroglobulinaemia. Creatinine 650. Congo
Red strongly positive with typical birefringence. No special stain
available.
Specimen:
H&E
Diagnostic categories: Score:
1 Amyloidosis 9.86
2 Waldenstrom's (amyloidosis mentioned in comments) 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.86
Secondary diagnoses and comments (if any):
Congo red*6. EM*5. Waldenstrom's?*4. Investigation of amyloid type*7.
Monoclonal cells in stroma?*1. Myeloma type cast too?*5.
Original report and further information (if any):
Amyloidosis secondary to lymphoproliferative disease.
Links to cases in this document:
Top
L 200
L 201
L 202
L 203
L 204
L 205
Last updated: 27 APR 03
Organiser:
Professor Peter Furness, PhD, FRCPath.
Clinical Sciences Laboratories
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk