National Renal Pathology E.Q.A. Scheme
Circulation E
This document gives information on individual cases in
circulation E of this scheme. It contains no personal details
of participants.
Cases included:
E 164
E 165
E 166
E 167
E 168
E 169
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: E
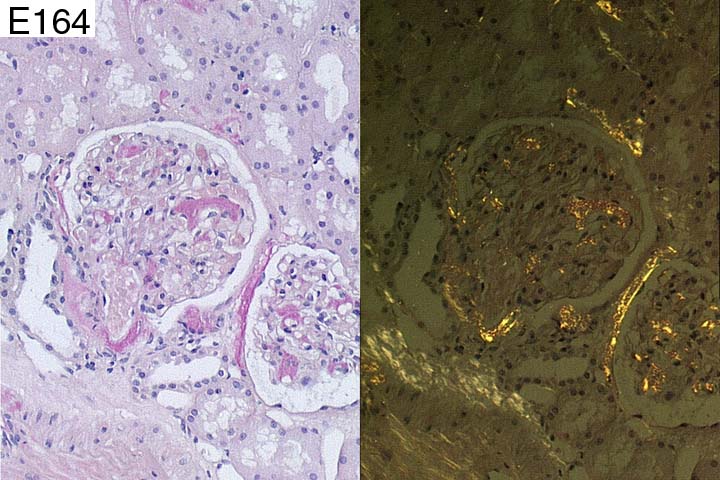
Case number: 164
....
Number of responses:76 . Date of analysis: 8 APR 01
Clinical:
Male, 64. Nephrotic syndrome. No underlying factors identified.
Specimen:
H&E, silver, MSB, Elastin, Sirius Red, PAS
Diagnostic categories: Score:
1 Amyloidosis 9.87
2 Diabetic glomerulosclerosis (but do Congo red) 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.87
Secondary diagnoses and comments (if any):
Test for amyloid type*15 Congo red*1. Myeloma screen*3. MSB artefactual
positive?*1. EM*4. Hypertension too*1. Exclude diabetes*1. Immono/em to
esclude other causes of nephrotic syndrome*1.
Original report and further information (if any):
Amyloidosis. CR positivity was resistant to permanganate bleach, so
probably AL type.
Circulation: E
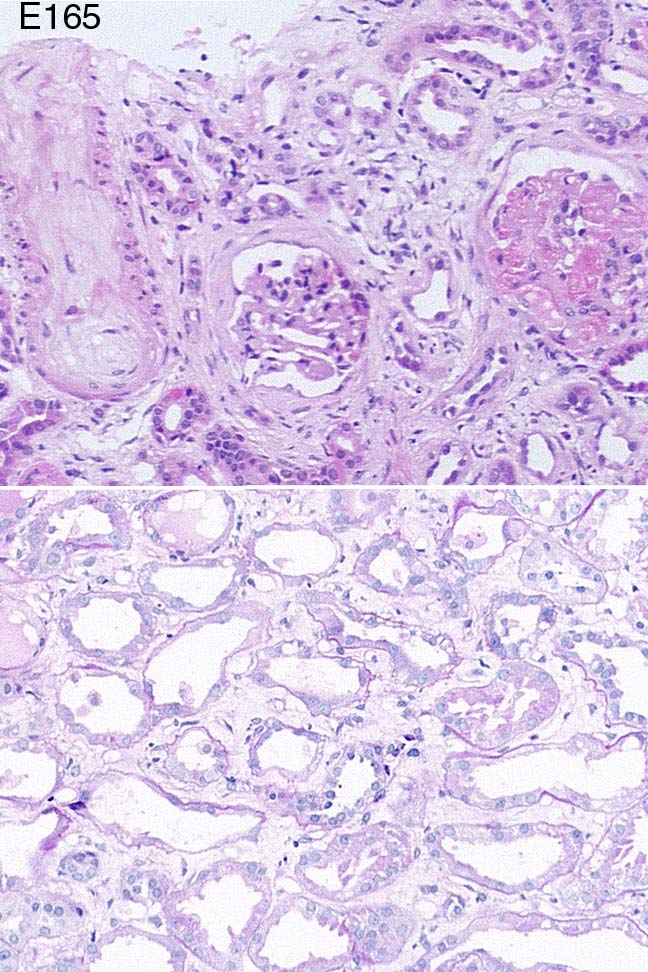
Case number: 165
....
Number of responses:76 . Date of analysis: 8 APR 01
Clinical:
64y.o. woman with ?scleroderma. 6 months hypertension, SOB, joint pains,
Raynaud's. Protein 0.78g/24h, nausea, peripheral oedema, +ve ANA 1:10,240.
Serum creatinine 95 to 203 over last 2 weeks.
Specimen:
H&E, PAS, Masson
Diagnostic categories: Score:
1 Hypertension 0.00
2 Systemic sclerosis / scleroderma 6.43
3 Hypertension/scleroderma 2.37
4 Mixed connective tissue disease 0.13
5 Vasculitis 0.13
6 Focal segmental proliferative Gn 0.13
7 Microangiopathy/HUS/TTP 0.41
8 Lupus nephritis 0.26
9 Mesangiocapillary Gn c/w scleroderma 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.43
Secondary diagnoses and comments (if any):
Capillary thrombosis noted*2. Chronic TIN*1. Blood pressure?*8. IF*6. EM*
3. Exclude SLE*2. Exclude antiphospholipid syundrome*1. ANCA*2. More
clinical info*2. Insufficient info. for diagnosis*2.
Original report and further information (if any):
Circulation: E
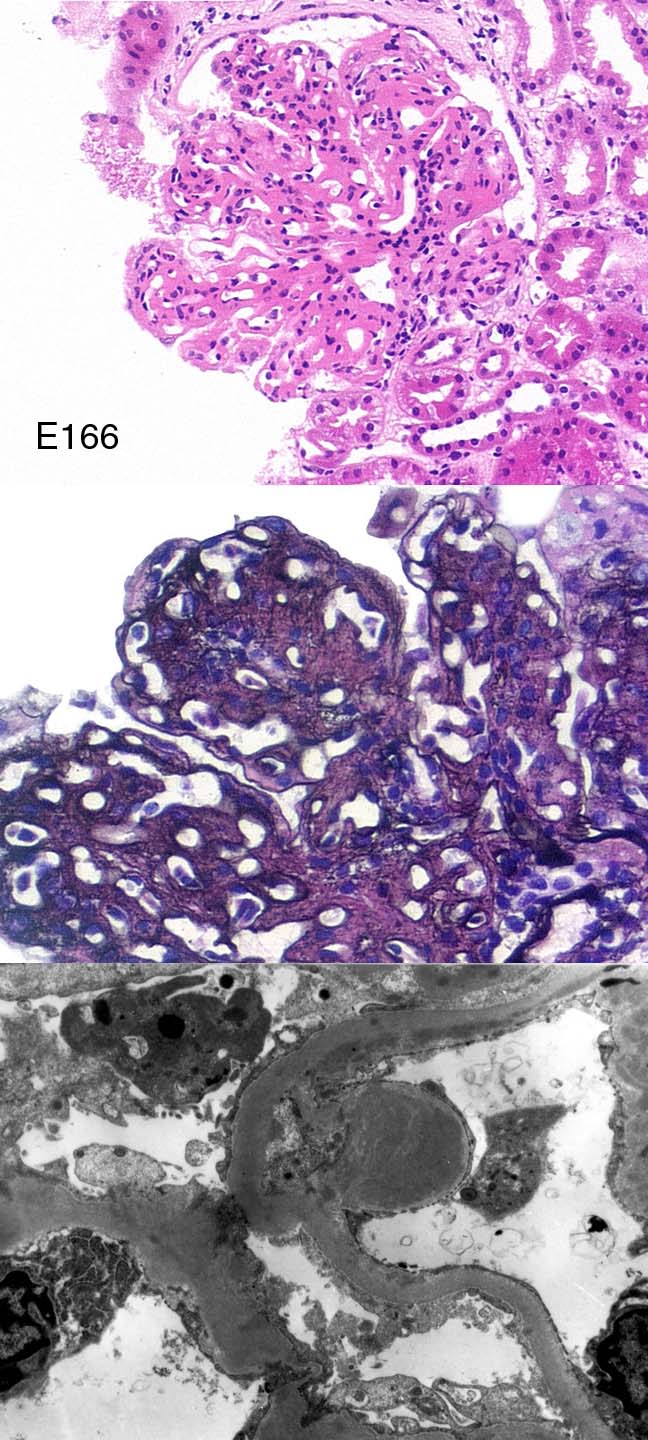
Case number: 166
....
Number of responses:76 . Date of analysis: 8 APR 01
Clinical:
Male, 23, nephrotic syndrome for 1/12, hypertension, microscopic haematuria.
Immunoperoxidase: C3+++ in expanded mesangial areas and capillary walls.
IgM+, C1q+, Fib+ in peripheral capillary walls only.
Specimen:
H&E, silver, EM x1.
Diagnostic categories: Score:
1 Mesangiocapillary glomerulonephritis type I (or III) 5.75
2 Mesangiocapillary glomerulonephritis type II (DDD) 1.58
3 Mesangiocapillary Gn NOS 2.50
4 Post-infectious Gn 0.04
5 Lupus nephritis 0.13
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 5.75
Secondary diagnoses and comments (if any):
Thick sections*1. Exclude 1ry causes of MPGn (cryo, lupus etc.)*10. Better
EM*4. Autoantibodies?*1.C3Nef?*1. Complement levels?*1. Hepatitis C
status?*2. Congo red*1.
Original report and further information (if any):
Membranoproliferative glomerulonephritis type I
Circulation: E
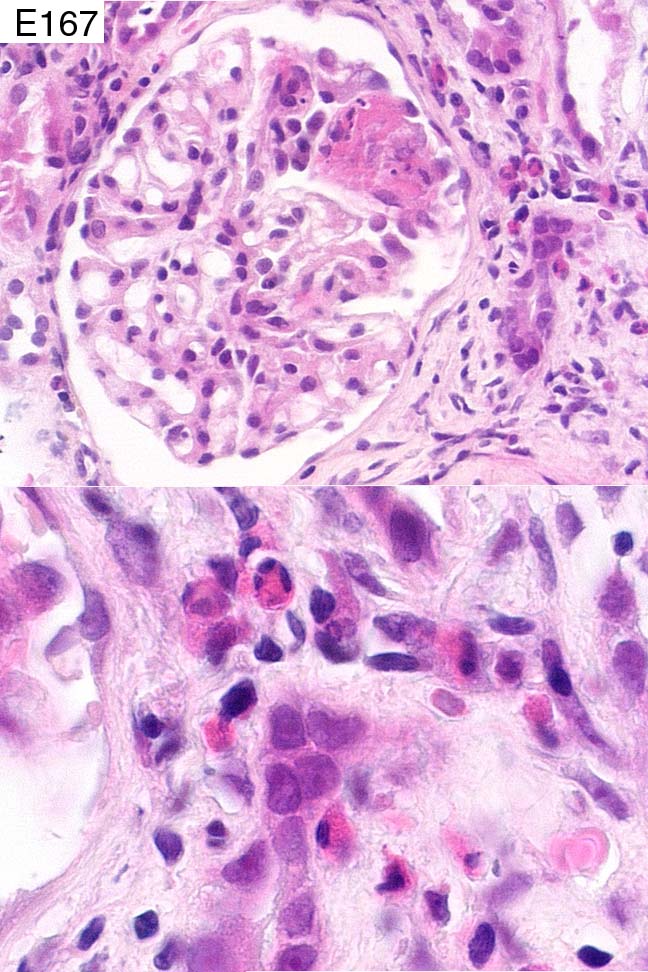
Case number: 167
....
Number of responses:76 . Date of analysis: 8 APR 01
Clinical:
79 y.o female presenting with acute renal failure and general malaise. ANCA
was positive and there was blood eosinophilia. 40 year history of asthma.
Immuno. showed non-specific staining in abnormal glomerular segments only.
No glomeruli for e.m.
Specimen:
H&E
Diagnostic categories: Score:
1 Vasculitis c/w Churg Strauss syndrome 6.55
2 Vascuitis; Churg Strauss not mentioned 2.89
3 Tubulointerstitial nephritis and old crescents 0.13
4 Pauci-immune focal segmental Gn 0.13
5 Crescentic glomerulonephritis 0.13
6 Focal segmental proliferative Gn ?vasculitic 0.13
7 Hypereosinophilic syndrome 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.55
Secondary diagnoses and comments (if any):
Silver*2. IF*1. Fibrin stain*1. ANCA type?*2. Poor/pale section*5. Need
specials *2. Inadequate for EQA*1.
Original report and further information (if any):
Churg-Strauss syndrome. Treated with cyclophosphamide and steroids;
improved, off dialysis, but dies a few months later - apparently of
ischaemic heart disease (no PM).
Circulation: E
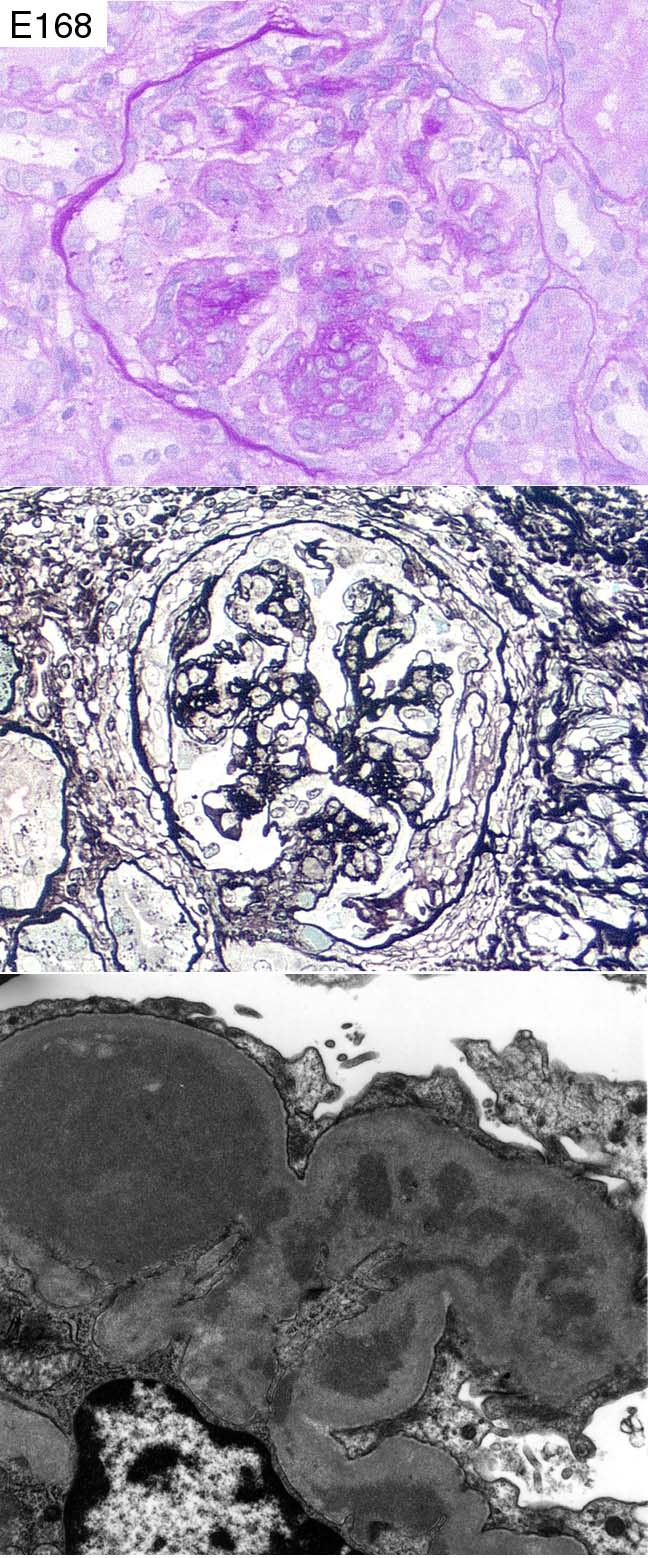
Case number: 168
....
Number of responses:76 . Date of analysis: 8 APR 01
Clinical:
Female aged 54. Clinical history: 'Nephrotic/Nephritic'. No other info!
IF: IgG+, A+++, M+, C3+++, C1q+, all diffuse granular mesangial with some
peripheral staining.
Specimen:
PAS, silver, EM x2
Diagnostic categories: Score:
1 IgA nephropathy / HSP 6.99
2 MPGn type I 0.79
3 Mixed pattern glomerulopathy ?SLE 0.41
4 MPGn ? lupus 0.92
5 Lupus nephritis 0.89
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.99
Secondary diagnoses and comments (if any):
Need H&E*8. Check autoantibodies / lupus serology*15. ANCA?*1. ?cryo.*1.
Unsuitable for EQA*4.
Original report and further information (if any):
Henoch-Schonlein purpura. Subsequently improved and remains well,
creatinine 89.
Circulation: E
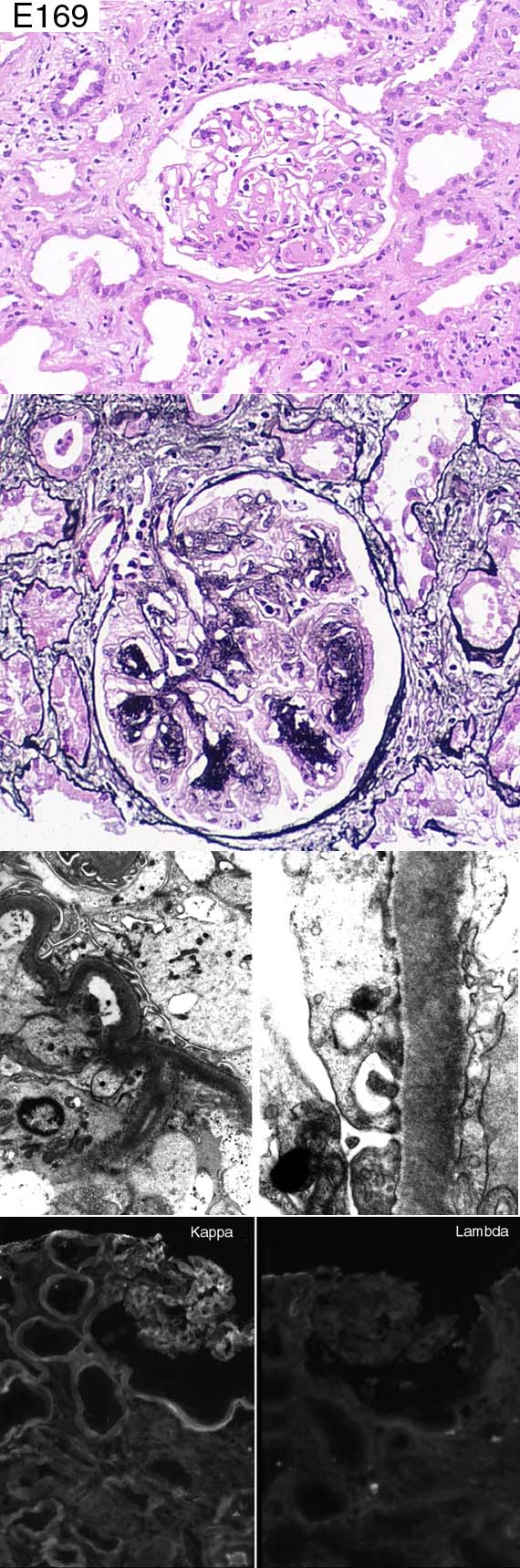
Case number: 169
....
Number of responses:62 . Date of analysis: 8 APR 01
Clinical:
FOR INTEREST NOT PERSONAL ASSESSMENT. 62y.o. woman. Hypercalcaemia, ?
sarcoidosis, responded to steriod therapy. Serum immunoelectrophoresis no
monoclonal band. Declining renal function; creatinine 200 to 450 over 2
months. Interstitial nephritis? Exclude RPGn.
Specimen:
H&E, photos of silver, EMx2, IFx2.
Diagnostic categories: Score:
1 Light chain nephropathy 8.47
2 Immunotactoid Gn 0.24
3 Mesangiocapillary Gn 0.65
4 Myeloma 0.16
5 FSGS 0.00
6 Monoclonal immunoglobulin deposition disease 0.32
7 Fibrillary glomerulopathy 0.16
8 Diabetes 0.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 8.47
Secondary diagnoses and comments (if any):
Negative IEP does not exclude light chain nephropathy*2. Repeat IEP*2.
Underlying lymphoproliferative disorder?*1. Skeletal survey?*1. Check no
amyloid*3. Cast nephropathy too*1.
(Photos missing*1)
Original report and further information (if any):
Light chain nephropathy. Subsequently found to have low levels of kappa
light chains in urine. Bone marrow showed excess of kappa +ve plasma
cells.
Links to cases in this document:
Top
E 164
E 165
E 166
E 167
E 168
E 169
Last updated: 8 APR 01
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk