National Renal Pathology E.Q.A. Scheme
Circulation D
This document gives information on individual cases in
circulation D of this scheme. It contains no personal details
of participants.
Cases included:
D 158
D 159
D 160
D 161
D 162
D 163
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: D
Case number: 158
....
Number of responses:73 . Date of analysis: 8 APR 01
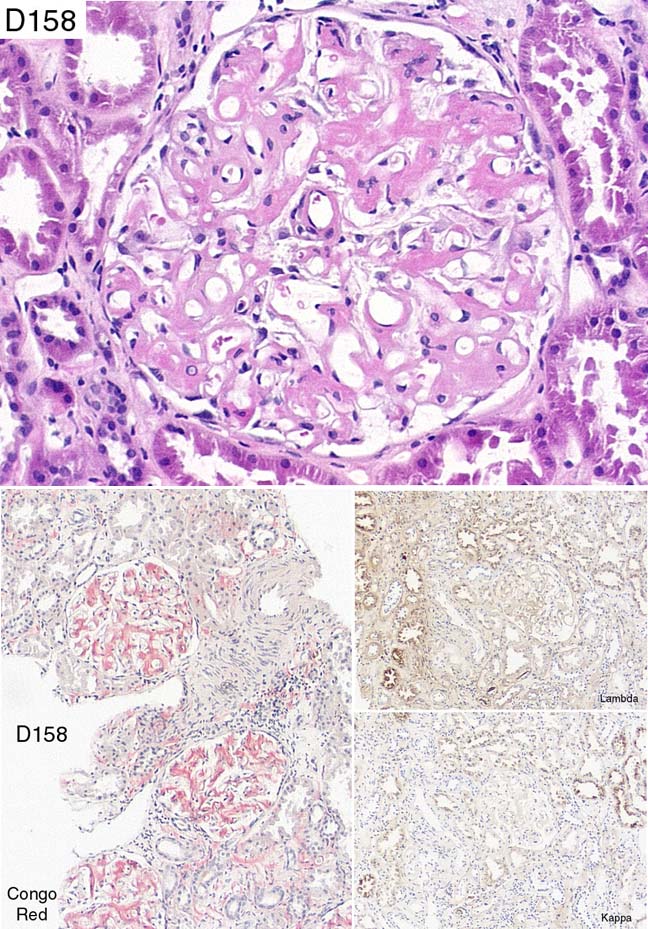
Clinical:
Unspecified neurodegenerative disease involving autoimmune nervous system,
gross oedema, proteinuria 5 gms, creatinine normal. ?Cause of nephrotic
syndrome. Male, 29 y.o. No material for EM or IF.
Specimen:
H&E, silver, images of immuno & Congo Red
Diagnostic categories: Score:
1 Amyloid ?familial amyloidotic polyneuropathy 0.96
2 Amyloid NOS / ? lambda 8.08
3 Amyloidosis ? hereditary disorder 0.96
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 8.08
Secondary diagnoses and comments (if any):
Tests for amyloid type*7. K and L not interpretable*6. Need to confirm
birefringence*3. EM to confirm*1. Cast nephropathy?*3. Bone marrow*1. ?
myeloma*8. Family history?*4. ?POEMS syndrome?*1.
Original report and further information (if any):
Amyloidosis. Subsequently found to have IgG lambda paraprotein 1g/litre;
bone marrow showed increased plasma cells. Treated symptomatically. Did
not attend last appointment .
Circulation: D
Case number: 159
....
Number of responses:73 . Date of analysis: 8 APR 01
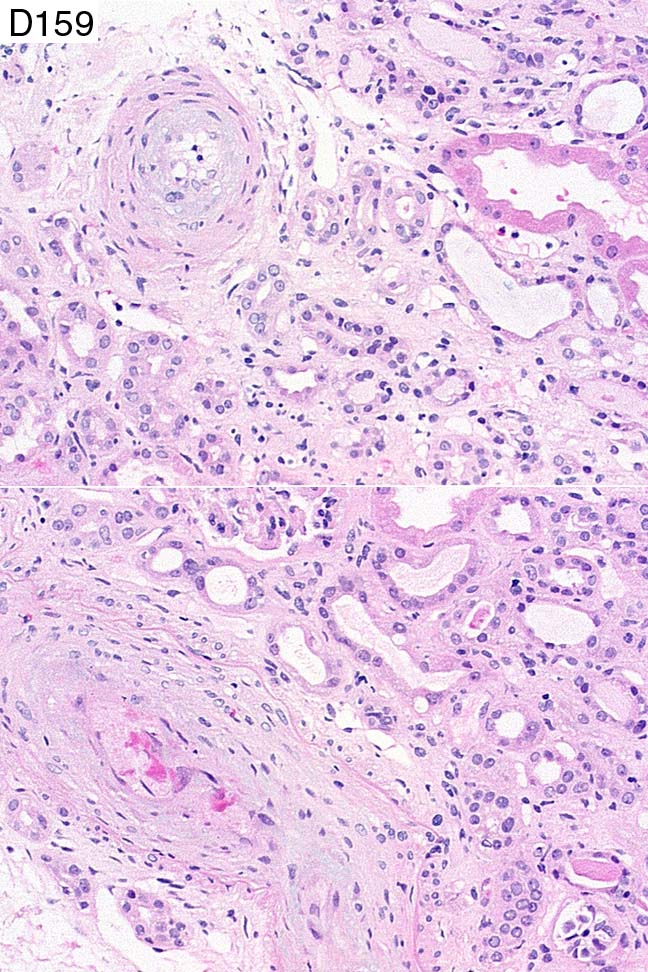
Clinical:
65 y.o. woman. Acute renal failure following loin pain and GI bleed. Also
Duke's C ca. ?interstitial nephritis ??ATN. Now anuric. ?MPGN.
Specimen:
H&E, PAAg
Diagnostic categories: Score:
1 Hypertension 1.37
2 Systemic sclerosis 0.55
3 Vascular changes of hypertension or systemic sclerosis 2.51
4 Vasculopathy - ?HT, ?SS, ?HUS/TTP etc 2.29
5 Thrombotic microangiopathy 0.78
6 Acute tubular necrosis 0.82
7 Proliferative / Membranoproliferative Gn 0.47
8 HUS 0.68
9 ATN / pre-renal ischaemia 0.53
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 3 with 2.51
Secondary diagnoses and comments (if any):
Secondary ATN*2. Blood pressure?*6. Clinical history *2. Drug history?*3.
2ry to Ca?*1. RBC fragmentation?*2. IF*5. EM*5. EVG*2. Section too pale*
4. Unsuitable for EQA*6.
Original report and further information (if any):
Circulation: D
Case number: 160
....
Number of responses:73 . Date of analysis: 8 APR 01
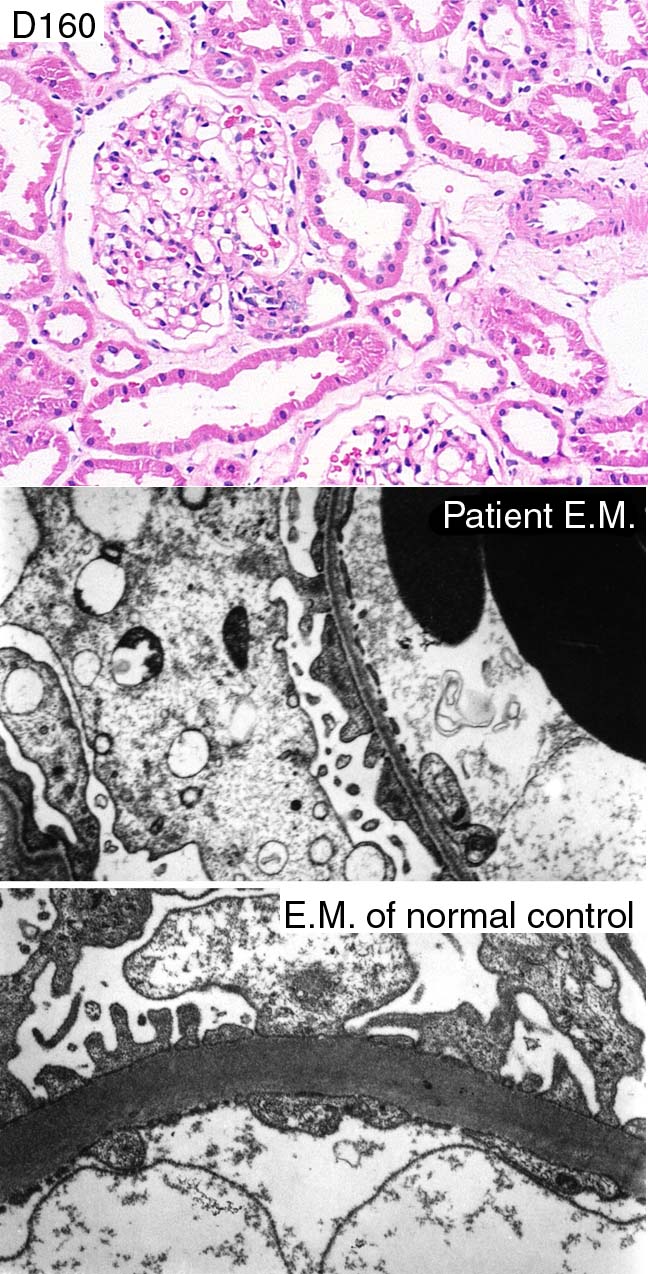
Clinical:
Female, 31, persistent microscopic haematuria, no proteinuria, normal renal
function, normal urological exam. Top EM (1026159) is typical; of patient.
NB LOWER EM IS CONTROL of normal GMB at same magnification (No. 1026169).
Specimen:
H&E, EM x2 (BUT SEE INFO ABOVE!!!)
Diagnostic categories: Score:
1 Thin membrane nephropathy / BFH 10.00
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 10.00
Secondary diagnoses and comments (if any):
Exclude early Alport's*7. More EM*1. Family history?*6. Immuno. to exclude
IgA*1. Exclude bleeding from lower urinary tract*1. Need scale*2.
Original report and further information (if any):
Thin glomerular basement membrane disease.
Circulation: D
Case number: 161
....
Number of responses:73 . Date of analysis: 8 APR 01
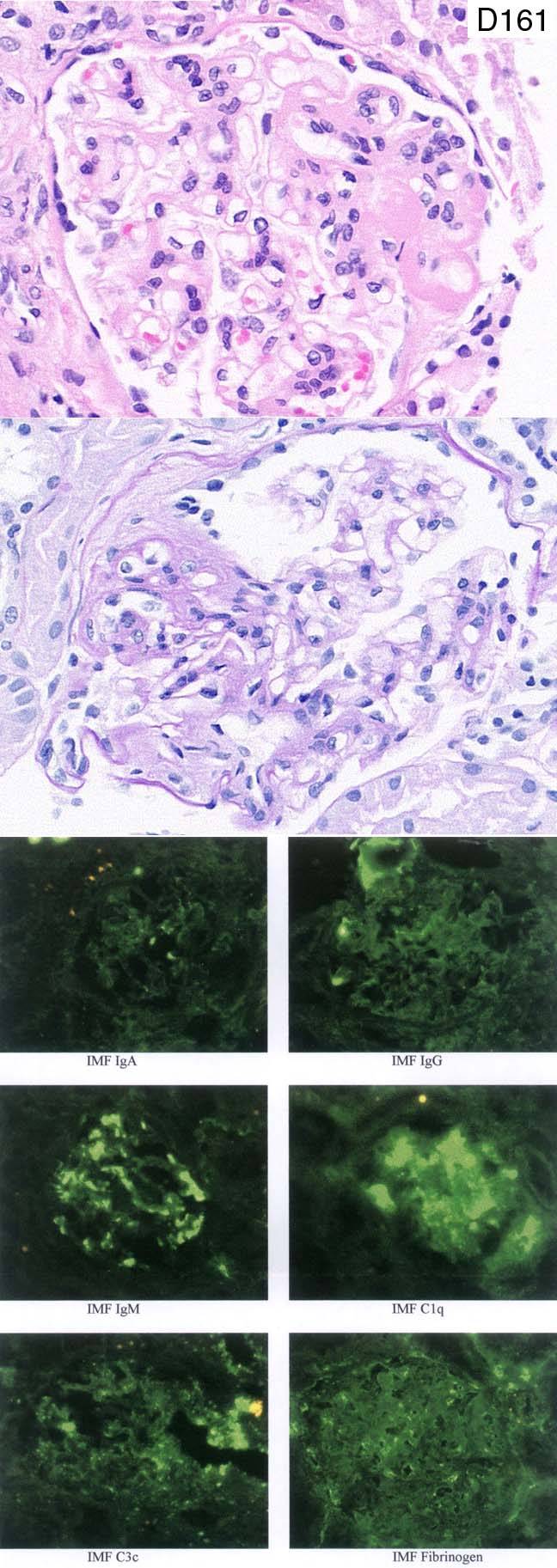
Clinical:
34 y.o man, nephrotic 1 month, 24h proteinuria 9.6g, alb. 26g/l, cholesterol
8.5 Oedema resolved on diuretics. BP 1324/80, creatinine 88. History of
bilateral uveitis 1984. First biopsy inadequate; treated pred. 60mg/day +
rimapril for 6 months. Proteinuria down only to 3 - 5g/24h so rebiopsy.
Creatinine remains 89.
Specimen:
H&E, PAS, IF images x6
Diagnostic categories: Score:
1 FSGS (Primary) 6.37
2 C1q nephropathy 0.47
3 IgM nephropathy 0.85
4 Mesangial proliferative glomerulonephritis 1.00
5 SLE 0.86
6 Focal segmental proliferative Gn. 0.14
7 Focal glomerulonephritis 0.14
8 Membranoproliferative Gn 0.14
9 Behcet's syndrome with 2ry amyloidosis 0.04
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 6.37
Secondary diagnoses and comments (if any):
Jokes about my typo. on systolic BP*several !!! EM*7. Silver*3. Secondary
to sarcoid?*2. ?Sjogren's / sicca syndrome*1. ?sarcoid*1. Lupus serology?*
10. Negative controls for IF needed*2. Amyloid stains*1. Insufficient for
EQA*2.
Original report and further information (if any):
Focal segmental glomerulosclerosis. No follow-up available.
Circulation: D
Case number: 162
....
Number of responses:73 . Date of analysis: 8 APR 01
Clinical:
76 year old man with acute renal failure. ESR 92mm/hr, Hb 7.7. IF
negative. No tissue for EM.
Specimen:
H&E, silver, PAS
Diagnostic categories: Score:
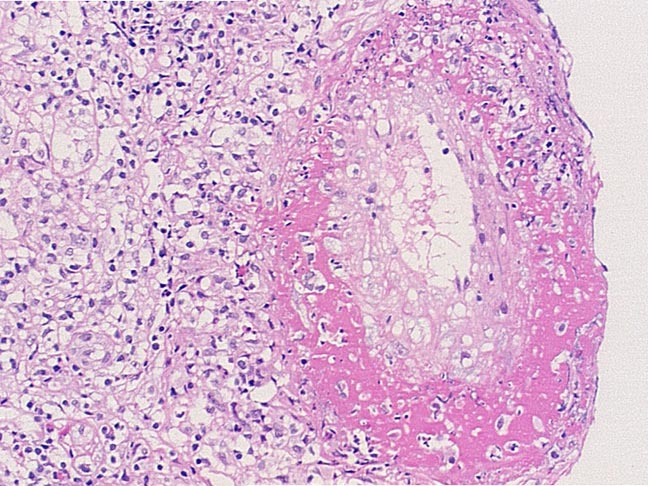
1 Necrotising Gn / Vasculitis 7.92
2 Vasculitis ?Churg Strauss 0.68
3 Wegener's 0.55
4 Polyarteritis 0.82
5 Accelerated hypertension 0.03
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 7.92
Secondary diagnoses and comments (if any):
ANCA (+/-type?)*25. Exclude lymphomatous infiltrate*2. MSB*1. Elastic
stain*1. Anti-GBM*2. Viral screen *1. Clinical info.*2. Blood pressure?*1.
Original report and further information (if any):
A severe medium and small vessel vasculitis, with 13% crescents, and a
diffuse interstitial nephritis.
Circulation: D
Case number: 163
....
Number of responses:62 . Date of analysis: 8 APR 01
Clinical:
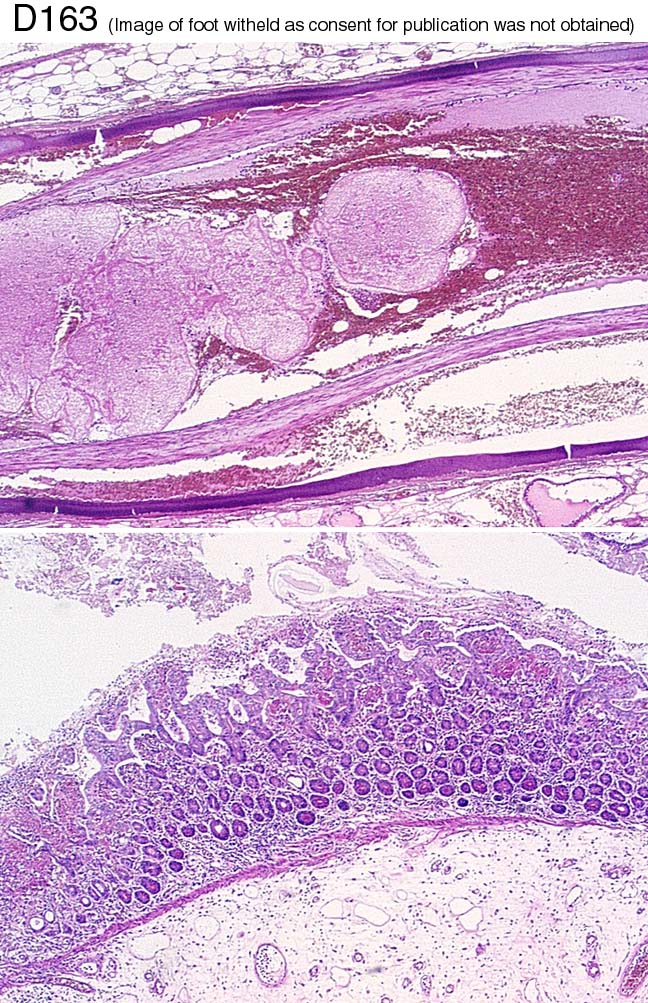
FOR INTEREST NOT SCORING 21 year old woman, developed CRF in teens.
Tertiary hyperparathyroidism; refused parathyroidectomy on advice of
homeopathic practitioner. CAPD peritonitis. Perforated bowel resected x2.
Abdominal wound would not heal. Died.
Specimen:
H&E of bowel & mesentery, PM photo of foot.
Diagnostic categories: Score:
1 'Calciphylaxix' 2.08
2 Vascular calcification (same as 1) 6.56
3 Inflammatory bowel disease 0.16
4 Ischaemic bowel 0.56
5 Sclerosing peritonitis 0.16
6 Scleroderma 0.05
7 Septic emboli / Aspergillosis? 0.32
8 Microangiopathy 0.08
9 Gastro-intestinal stromal tumour 0.02
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 2 with 6.56
Secondary diagnoses and comments (if any):
?CMV*1. ?ischaemia*1. ?cryoglobulin*1. Stains for organisms*1. Cause of
renal failure?*1.
Original report and further information (if any):
'Calcyphylaxix' (i.e. massive metastatic caclcification in vessels causing
poor tissue perfusion & failure to heal).
Links to cases in this document:
Top
D 158
D 159
D 160
D 161
D 162
D 163
Last updated: 8 APR 01
Organiser:
Dr Peter Furness, PhD, FRCPath.
Department of Pathology,
Clinical Sciences Building,
Leicester Royal Infirmary,
P. O. Box 65,
Leicester, U.K.
Tel: (0116)2584582
Fax: (0116) 2584573
Email:
pnf1@le.ac.uk