National Renal Pathology E.Q.A. Scheme
Circulation B
This document gives information on individual cases in
circulation B of this scheme. It contains no personal details
of participants.
Cases included:
B 290
B 291
B 292
B 293
B 294
B 295
End
A click on the  icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
icon should provide an image from the material
circulated.
Some of the images are composites - remember to scroll the image
to see parts beyond the bottom of your screen.
WARNING The image files associated with this
document are selected by the Organiser in an attempt to
illustrate the relevant features of the material which was
circulated in the EQA scheme. They are intended as an 'aide
memoire' for participants who may no longer have the slides for
review.
They are NOT intended as 'good examples' or as
teaching material. Some of the images may be chosen to
illustrate a feature which led some participants to a
wrong diagnosis.
Case Response Analysis
Circulation: B
Case number: 290
....
Number of responses:53 . Date of analysis: 18 JUL 08
Clinical:
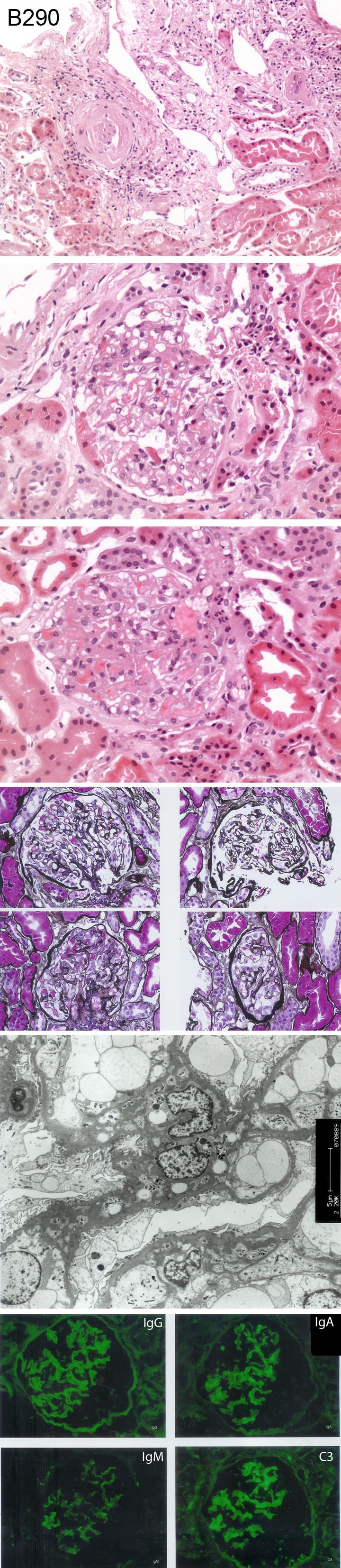
FOR EDUCATION AND INTEREST ONLY. Male, 34 years old. Presented with ankle
oedema for four weeks. Urea 5.3 mmol/L, creatinine 82 umol/L, Albumin 18
g/L, urine protein 5 g/day. Haematuria +. Clinical diagnosis nephrotic
syndrome. Direct immunofluorescence study is negative for fibrin and C1q
Specimen:
H&E, Photos of PASM, IMF and EM
Diagnostic categories: Score:
1 FSGS 0.92
2 Minimal change nephropathy 0.89
3 Mesangial proliferative glomerulonephritis 0.49
4 Lupus nephritis 2.26
5 IgA nephropathy 1.58
6 Simultaneous IgA and membranous Gn 0.09
7 Storage disorder 0.38
8 Cryoglobulinaemia 0.79
9 Dense deposit disease 0.57
10 Others- see below 2.02
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 4 with 2.26
Secondary diagnoses and comments (if any):
Odd IF pictures - ? exposure time?*1. Lupus serology*2. Congo red*1.
Insufficient material*1. Insufficient information*1. NEEDS STEROIDS!*1.
Other diagnoses (line 10): - HIVAN*3. Immune complex Gn NOS*1. Anti-GBM
nephritis*1. Light chain nephropathy*1.5. MCGntype I*1. Diabetes*1.
Membranous*1. Endothelial abnormality*0.2
Original report and further information (if any):
Minimal change nephrotic syndrome with co-incidental IgA nephropathy.
Circulation: B
Case number: 291
....
Number of responses:74 . Date of analysis: 18 JUL 08
Clinical:
Male, 65 years old. Seropositive rheumatoid arthritis and previous gold
treatment. Now nephritic (6g), albumin 10, creatinine 95 and normal blood
pressure. Congo red negative, EM of tubules normal.
Specimen:
H&E, PAMS, Photos of IF and EM
Diagnostic categories: Score:
1 Membranous glomerulonephritis 9.05
2 Gold-induced mebranous nephropathy 0.81
3 Membranoproliferative glomerulonephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.05
Secondary diagnoses and comments (if any):
Could be secondary to gold Rx?*22. Exclude SLE*4. Exclude malignancy*1.
Penicillamine too?*1. Exclude RVT*1. Diabetes too?*1.
Presumed typo. in clinical info. (nephritic / nephrotic)? Info given to me
really did say nephritic - PNF
Original report and further information (if any):
The overall appearances are consistent with a stage 1 � 2 membranous
glomerulonephritis in keeping with gold therapy.
Circulation: B
Case number: 292
....
Number of responses:74 . Date of analysis: 18 JUL 08
Clinical:
Male, 38 years old. Haematuria following URTI, with hypertension and
proteinuria. CKD: Creatinine 139, PCR 0.128 and eGFR 54. IgG negative.
Specimen:
H&E, PAMS, Photos of IF and EM
Diagnostic categories: Score:
1 IgA nephropathy 9.24
2 (Resolving) postinfectious Gn 0.62
3 Lupus nephritis (class II) 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.24
Secondary diagnoses and comments (if any):
Also cholesterol emboli*1. Cholesterol in tubules*1. Also hypertensive
change*2. Congo red*1. Exclude lupus*3. ?C1q nephropathy?*1.
Original report and further information (if any):
Overall appearances are those of active IgA nephropathy associated with
several poor prognostic features including segmental and diffuse peripheral
capillary wall lesions, hyaline deposition and hypertensive changes.
Circulation: B
Case number: 293
....
Number of responses:74 . Date of analysis: 18 JUL 08
Clinical:
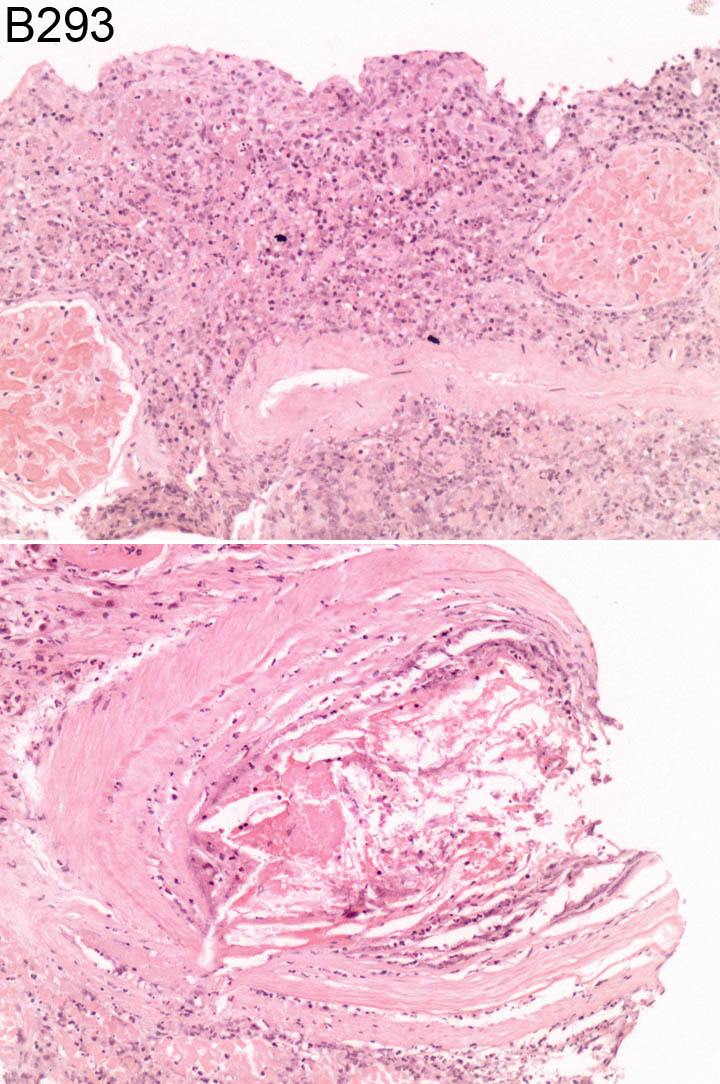
Male, 72 years old. Rapidly progressive renal failure. Creatinine 130 (Feb
2007) rising to 500 (presently). Dipstik urine: Blood +++, protein +++.
Also has rash on legs and feet. Recently investigated for microscopic
haematuria. Know AAA and hypertension. ANA -ve, ANCA -ve, anti-GBM -
negative, C3 and C4 normal.
Specimen:
H&E
Diagnostic categories: Score:
1 (Necrosis due to) atheroembolism 9.46
2 Infarction due to thromboembolism 0.14
3 Infarction secondary to thrombosis 0.14
4 Infarction 0.27
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.46
Secondary diagnoses and comments (if any):
Peripheral eosinophilia?*1. Any prior surgery / angiography?*2. Previous
anticoagulation?*1.
Original report and further information (if any):
Infarction associated with cholesterol emboli.
Circulation: B
Case number: 294
....
Number of responses:74 . Date of analysis: 18 JUL 08
Clinical:
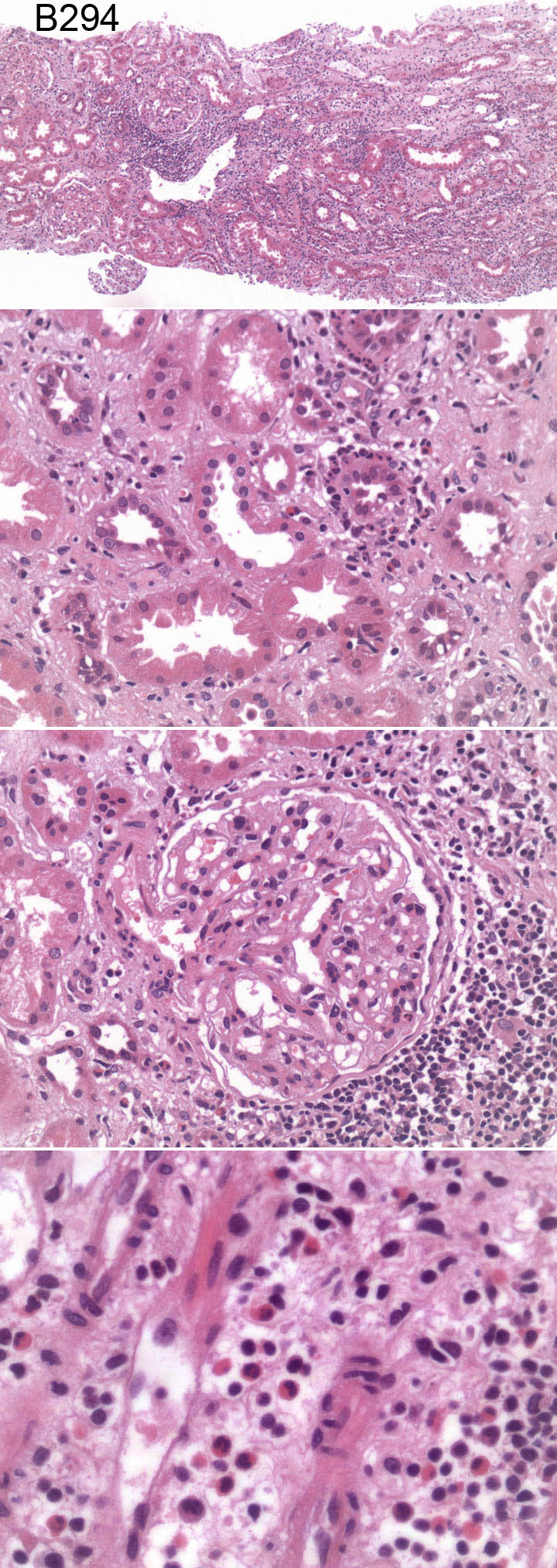
Female, 34 years old. Presented with nausea and dehydration. Acute renal
failure, scanty blood and protein in urine. Renal function failed to
improve with fluids. ANCA and anti-GBM antibodies negative. Normal kidneys
on ultrasound. IF negative. EM not done.
Specimen:
H&E
Diagnostic categories: Score:
1 Acute tubulointerstitial nephritis 9.16
2 Acute tubular necrosis 0.70
3 Acute pyelonephritis 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.16
Secondary diagnoses and comments (if any):
Drug history?*33. EM*1. A few neutrophils - exclude infection*3. Thick BMs,
exclude diabetes*1.
Original report and further information (if any):
The appearance is of tubulo-interstitial nephritis. The presence of
eosinophils suggests a possible allergic/idiosyncratic cause. The process
appears to be predominantly acute, but the presence of some early
interstitial fibrosis and tubule collapse suggests that there may already
be some slight irreversible scarring. Given steriods; improved.
Circulation: B
Case number: 295
....
Number of responses:74 . Date of analysis: 18 JUL 08
Clinical:
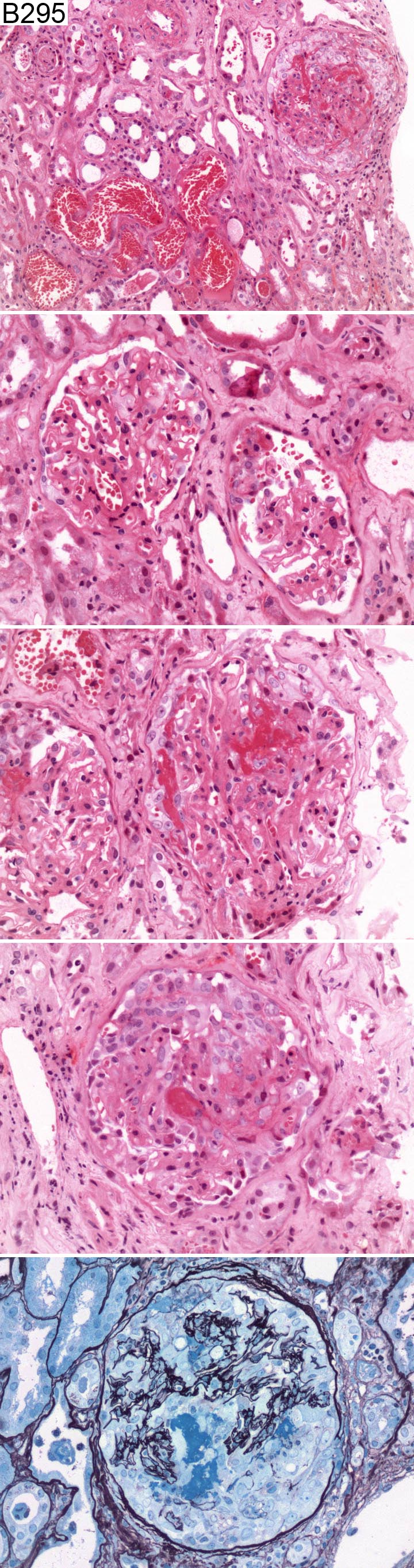
Male, 63 years old. Haemoptysis, ANCA strongly positive with rapidly
progressive renal impairment. Immunofluorescence - minor to moderate
deposition of C3 in all seven glomeruli with minor associated IgG staining.
No IgA or IgM staining. The immunofluorescent features were regarded as
non-specific. Electron microscopy - increased mesangial matrix, mild foot
process fusion, no deposits identified.
Specimen:
H&E, Silver
Diagnostic categories: Score:
1 Pauci-immun /vasculitic/ANCA-assoc. crescentic Gn 9.86
2 Necrotising Gn with crescents 0.14
Asterisks (if any) indicate dangerous diagnoses.
Highest scoring diagnosis was 1 with 9.86
Secondary diagnoses and comments (if any):
Presumably Wegener's*17. Also ATN*3. ANCA type?*6. Check anti-GBM
serology*3.
Original report and further information (if any):
Links to cases in this document:
Top
B 290
B 291
B 292
B 293
B 294
B 295
Last updated: 18 JUL 08
Organiser:
Professor Peter Furness, PhD, FRCPath.
Department of Pathology
Leicester General Hospital
Gwendolen Road
Leicester
LE5 4PW, U.K.
Tel: (0116)2584582
Fax: (0116) 2584582
Email:
peter.furness@le.ac.uk